A novel coronavirus is a new coronavirus that has not been previously identified. The virus causing coronavirus disease 2019 (COVID-19), is not the same as the coronaviruses that commonly circulate among humans and cause mild illness, like the common cold.
A diagnosis with coronavirus 229E, NL63, OC43, or HKU1 is not the same as a COVID-19 diagnosis. Patients with COVID-19 will be evaluated and cared for differently than patients with common coronavirus diagnosis.
The COVID‑19 pandemic, also known as the coronavirus pandemic, is an ongoing pandemic of coronavirus disease 2019 (COVID‑19) caused by severe acute respiratory syndrome coronavirus 2 (SARS‑CoV‑2). The disease was first identified in December 2019 in Wuhan, China. The World Health Organization declared the outbreak a Public Health Emergency of International Concern on 30 January 2020 and a pandemic on 11 March. As of 16 September 2020, more than 29.6 million cases have been reported in 188 countries and territories, resulting in more than 936,000 deaths; more than 20.1 million people have recovered.
This timeline provides information about select moments in the COVID-19 pandemic in the United States and around the world beginning from its known origins to today.
In 2003, a coronavirus that killed one in every 10 people it infected emerged from China and spread through several countries. Then, within eight months of being detected, it seemingly vanished. RFE/RL asked one of the world’s leading virologists why.
Paramedics tend to a man suspected of suffering from severe acute respiratory syndrome (SARS) after he collapses in Wuhan, China.
When this photo was taken on April 29, 2003, the world was in the midst of what threatened to become the first pandemic of the 21st century. SARS was a mysterious new coronavirus that killed some 10 percent of people it infected, mostly as a result of patients’ lungs clogging with fluid.
[...]
In late 2002, SARS began its deadly spree after a coronavirus that is thought to have thrived in bats infected a civet cat, which in turn infected a person in southern China. Viruses can be passed from animals to people through inhaling an animal’s breath, eating food contaminated with animal feces, or exchanging bodily fluids -- as might happen when a butcher works with a cut hand.
[...]
Such “spillover infections”between species are commonplace, but the coronavirus that infected SARS patient zero in 2002 developed a trick that could wreak global havoc: the ability to jump easily between humans.
[...]
As dozens, then hundreds, of people in China were stricken down by the frightening new disease, the country’s ruling Communist Party began a Chernobyl-like cover-up of the unfolding crisis. Doctors were muzzled, and travel continued unchecked.
[...]
Metropole hotel guests from Vietnam and Singapore also carried the virus back to their home countries, sparking fresh SARS outbreaks and further global spread, as well as some drastic containment measures. By June 2003, at least 774 people had been killed by the virus. And then it stopped.
[...]
Virology Professor John Oxford tells RFE/RL the reason the 2003 SARS outbreak fizzled out with less than 1 percent of the deaths of the COVID-19 outbreak so far is largely down to luck.
"I think the two viruses are very different," Oxford says. "We were very lucky in this regard with SARS in 2003. It was nothing like as spreadable as [the COVID-19 coronavirus]." And with strict containment measures enacted in most of the countries where it appeared, he says, "in the end it ran out of people to infect, it just ran out of steam."
[...]
rferl.org [2022-02-06] By Amos Chapple, April 11, 2020 link archive General
Most adults showed preexisting antibody reactivity against SARS-CoV-2, 90% uninfected adults showed antibody reactivity against spike protein, receptor-binding domain, Nucleocapsid, N-terminal domain
‘Preexisting cross-reactivity to SARS-CoV-2 occurs in the absence of prior viral exposure. However, this has been difficult to quantify at the population level due to a lack of reliably defined seroreactivity thresholds. Using an orthogonal antibody testing approach, we estimated that about 0.6% of nontriaged adults from the greater Vancouver, Canada, area between May 17 and June 19, 2020, showed clear evidence of a prior SARS-CoV-2 infection, after adjusting for false-positive and false-negative test results.
Using a highly sensitive multiplex assay and positive/negative thresholds established in infants in whom maternal antibodies have waned, we determined that more than 90% of uninfected adults showed antibody reactivity against the spike protein, receptor-binding domain (RBD), N-terminal domain (NTD), or the nucleocapsid (N) protein from SARS-CoV-2.
This seroreactivity was evenly distributed across age and sex, correlated with circulating coronaviruses’ reactivity, and was partially outcompeted by soluble circulating coronaviruses’ spike. Using a custom SARS-CoV-2 peptide mapping array, we found that this antibody reactivity broadly mapped to spike and to conserved nonstructural viral proteins. We conclude that most adults display preexisting antibody cross-reactivity against SARS-CoV-2, which further supports investigation of how this may impact the clinical severity of COVID-19 or SARS-CoV-2 vaccine responses.’
More information on the author Dr. Paul Alexander
palexander.substack.com [2022-10-05] Dr. Paul Alexander, October 4, 2022 link archive General
More information on Coronavirus Research/Studies prior to the 2020 pandemic
- Cases, Hospitalizations, Deaths -
See section on COVID-19 Statistics (Cases, Hospitalizations & Deaths)
At a time when everyone needs better information, from disease modelers and governments to people quarantined or just social distancing, we lack reliable evidence on how many people have been infected with SARS-CoV-2 or who continue to become infected. Better information is needed to guide decisions and actions of monumental significance and to monitor their impact.
Draconian countermeasures have been adopted in many countries. If the pandemic dissipates — either on its own or because of these measures — short-term extreme social distancing and lockdowns may be bearable. How long, though, should measures like these be continued if the pandemic churns across the globe unabated? How can policymakers tell if they are doing more good than harm?
statnews.com [June 4, 2020] By JOHN P.A. IOANNIDIS, MARCH 17, 2020 link archive General
The following interview with Norman Fenton by David Marks presents a comprehensive overview of how pandemic data was skewed to serve the interests of Big Pharma and Government agendas. It is from a new website just launched by Children’s Health Defense, called the Community Forum. In addition to this piece, the Forum will have a number of informative articles and information about advocating and organizing for change.
[...]
Fenton: A good example of how we used Bayesian analysis was to answer the question: Do I, or do I not, have the SARS-CoV-2 (COVID) virus? And specifically, if I'm asymptomatic, what is the probability that I might have the virus? Answering this question correctly was the focus of one of our first inquiries.
Suppose that at a given time there is data available suggesting that, in the general population, one in a thousand asymptomatic people were likely to have the virus. Such data was never confirmed of course, the infection rate varied over time, but I will use it to explain the Bayesian reasoning.
If I take a PCR test and it’s positive but I’m not feeling ill, I would want to know if I really have the virus. In other words, if I am one — of the one-in-a-thousand people — who is asymptomatic but carrying the virus, I’d want to know the accuracy of the test. There weren’t any reliable studies about the reliability of the PCR test, but the public was assured these tests were very accurate. Let’s suppose there was only a one-in-a-hundred chance that someone who doesn't have the virus will test positive — a 1% false positive rate. Then conversely, if I don't have the virus, there's a 99% chance of a negative test. With this information most people assumed if you tested positive you almost certainly had COVID. But that is not the case.
Think about a group of 10,000 asymptomatic people getting tested. Because we are assuming one-in-a-thousand asymptomatic people have the virus, that means about 10 of the 10,000 really have the virus. Let’s also assume these genuinely infected people test positive. Then we are left with just under 10,000 people — 9990, who do not have the virus. But a PCR test with only a 1%false positive rate still means that about 100 of these people would falsely test positive. So in total there are 110 people testing positive of whom we know only 10 will actually become ill from the virus. So, the actual probability that you've got the virus if you test positive is closer to 10%. This means that with reasonable assumptions about the underlying infection rate and test accuracy, the PCR test used as a standard for life-impacting decisions and mandates, had a 99% inaccuracy rate for asymptomatic people testing positive.
The confusion lies with the incorrect assumption that even if you don’t have symptoms of the virus, that the possibility of a false positive in the PCR test is only 1%. As more accurate calculations based on reliable data show, that is clearly not the case. To assume these probabilities are equal is known as the fallacy of the transposed conditional. In the courtroom, when DNA evidence is misinterpreted, it’s called the prosecutor's policy. Those contradictory figures should have raised important questions — it’s not that complicated — it can be presented in a confusing way, but scientists who knew better ignored this data.
Forum: Have the results of that comparative data been confirmed by other studies?
Fenton: We looked at the numbers from a study at Cambridge University where they tested several thousand asymptomatic students for the virus over weeks using pooled PCR testing. And during that period what they found was that very few students tested positive. In fact, over the period, only 43 of the 10,394 tests were positive.
However, unlike what happens in PCR testing in the general population, they did a second confirmatory test on each of the same samples that tested positive. They applied this more reliable, approved standard, where two positives were needed for confirmation; if either one was negative, it meant nobody in the pooled sample was infected. They found 36 out of the 43 samples that had tested positive, when re-tested afterwards, showed negative. So, what they saw was 84% of asymptomatic students showing a positive result on the initial test didn't have the virus, confirming a very high inaccuracy rate.
[...]
rwmalonemd.substack.com [2022-11-22] David Marks, Norman Fenton via Robert Malone's substack, November 21, 2022 link archive General
ATLANTA, Ga. (WEYI) - The Centers for Disease Control released information showing how many people who died from COVID-19 had comorbidities or underlying conditions as they are sometimes referred to by doctors.
According to the CDC, comorbidity is defined as: " more than one disease or condition is present in the same person at the same time. Conditions described as comorbidities are often chronic or long-term conditions. Other names to describe comorbid conditions are coexisting or co-occurring conditions and sometimes also “multimorbidity” or “multiple chronic conditions."
Comorbidity and underlying conditions can both be used to describe conditions that exist in one person at the same time. These can also contribute to a persons death who has been diagnosed with COVID-19.
Table 3 shows the types of health conditions and contributing causes mentioned in conjunction with deaths involving coronavirus disease 2019 (COVID-19). For 6% of the deaths, COVID-19 was the only cause mentioned. For deaths with conditions or causes in addition to COVID-19, on average, there were 2.6 additional conditions or causes per death.
The CDC says people need to always social distance and perform best practices when it comes to staying safe during the COVID-19 pandemic.
Question What are the characteristics, clinical presentation, and outcomes of patients hospitalized with coronavirus disease 2019 (COVID-19) in the US?
Findings In this case series that included 5700 patients hospitalized with COVID-19 in the New York City area, the most common comorbidities were hypertension, obesity, and diabetes. Among patients who were discharged or died (n = 2634), 14.2% were treated in the intensive care unit, 12.2% received invasive mechanical ventilation, 3.2% were treated with kidney replacement therapy, and 21% died.
Meaning This study provides characteristics and early outcomes of patients hospitalized with COVID-19 in the New York City area.
Abstract
Importance There is limited information describing the presenting characteristics and outcomes of US patients requiring hospitalization for coronavirus disease 2019 (COVID-19).
Objective To describe the clinical characteristics and outcomes of patients with COVID-19 hospitalized in a US health care system.
[...]
Results A total of 5700 patients were included (median age, 63 years [interquartile range {IQR}, 52-75; range, 0-107 years]; 39.7% female). The most common comorbidities were hypertension (3026; 56.6%), obesity (1737; 41.7%), and diabetes (1808; 33.8%). At triage, 30.7% of patients were febrile, 17.3% had a respiratory rate greater than 24 breaths/min, and 27.8% received supplemental oxygen. The rate of respiratory virus co-infection was 2.1%. Outcomes were assessed for 2634 patients who were discharged or had died at the study end point. During hospitalization, 373 patients (14.2%) (median age, 68 years [IQR, 56-78]; 33.5% female) were treated in the intensive care unit care, 320 (12.2%) received invasive mechanical ventilation, 81 (3.2%) were treated with kidney replacement therapy, and 553 (21%) died. As of April 4, 2020, for patients requiring mechanical ventilation (n = 1151, 20.2%), 38 (3.3%) were discharged alive, 282 (24.5%) died, and 831 (72.2%) remained in hospital. The median postdischarge follow-up time was 4.4 days (IQR, 2.2-9.3). A total of 45 patients (2.2%) were readmitted during the study period. The median time to readmission was 3 days (IQR, 1.0-4.5) for readmitted patients. Among the 3066 patients who remained hospitalized at the final study follow-up date (median age, 65 years [IQR, 54-75]), the median follow-up at time of censoring was 4.5 days (IQR, 2.4-8.1).
Conclusions and Relevance This case series provides characteristics and early outcomes of sequentially hospitalized patients with confirmed COVID-19 in the New York City area.
[...]
jamanetwork.com [2022-10-12] Safiya Richardson, Jamie S. Hirsch, Mangala Narasimhan, ..., Karina W. Davidson, April 22, 2020 link archive General
Objective: To estimate the infection fatality rate of coronavirus disease 2019 (COVID-19) from seroprevalence data.
Methods: I searched PubMed and preprint servers for COVID-19 seroprevalence studies with a sample size ≥ 500 as of 9 September 2020. I also retrieved additional results of national studies from preliminary press releases and reports. I assessed the studies for design features and seroprevalence estimates. I estimated the infection fatality rate for each study by dividing the cumulative number of COVID-19 deaths by the number of people estimated to be infected in each region. I corrected for the number of immunoglobin (Ig) types tested (IgG, IgM, IgA).
Findings: I included 61 studies (74 estimates) and eight preliminary national estimates. Seroprevalence estimates ranged from 0.02% to 53.40%. Infection fatality rates ranged from 0.00% to 1.63%, corrected values from 0.00% to 1.54%. Across 51 locations, the median COVID-19 infection fatality rate was 0.27% (corrected 0.23%): the rate was 0.09% in locations with COVID-19 population mortality rates less than the global average (< 118 deaths/million), 0.20% in locations with 118-500 COVID-19 deaths/million people and 0.57% in locations with > 500 COVID-19 deaths/million people. In people younger than 70 years, infection fatality rates ranged from 0.00% to 0.31% with crude and corrected medians of 0.05%.
Conclusion: The infection fatality rate of COVID-19 can vary substantially across different locations and this may reflect differences in population age structure and case-mix of infected and deceased patients and other factors. The inferred infection fatality rates tended to be much lower than estimates made earlier in the pandemic.
The infection fatality rate (IFR) of COVID-19 among non-elderly people in the absence of vaccination or prior infection is important to estimate accurately, since 94% of the global population is younger than 70 years and 86% is younger than 60 years. In systematic searches in SeroTracker and PubMed (protocol: https://osf.io/xvupr), we identified 40 eligible national seroprevalence studies covering 38 countries with pre-vaccination seroprevalence data. For 29 countries (24 high-income, 5 others), publicly available age-stratified COVID-19 death data and age-stratified seroprevalence information were available and were included in the primary analysis. The IFRs had a median of 0.035% (interquartile range (IQR) 0.013 - 0.056%) for the 0-59 years old population, and 0.095% (IQR 0.036 - 0.125%,) for the 0-69 years old. The median IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years, 0.011% at 30-39 years, 0.035% at 40-49 years, 0.129% at 50-59 years, and 0.501% at 60-69 years. Including data from another 9 countries with imputed age distribution of COVID-19 deaths yielded median IFR of 0.025-0.032% for 0-59 years and 0.063-0.082% for 0-69 years. Meta-regression analyses also suggested global IFR of 0.03% and 0.07%, respectively in these age groups. The current analysis suggests a much lower pre-vaccination IFR in non-elderly populations than previously suggested. Large differences did exist between countries and may reflect differences in comorbidities and other factors. These estimates provide a baseline from which to fathom further IFR declines with the widespread use of vaccination, prior infections, and evolution of new variants.
Highlights *Across 31 systematically identified national seroprevalence studies in the pre-vaccination era, the median infection fatality rate of COVID-19 was estimated to be 0.035% for people aged 0-59 years people and 0.095% for those aged 0-69 years.
*The median IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years, 0.011% at 30-39 years, 0.035% at 40-49 years, 0.129% at 50-59 years, and 0.501% at 60-69 years.
*At a global level, pre-vaccination IFR may have been as low as 0.03% and 0.07% for 0-59 and 0-69 year old people, respectively.
*These IFR estimates in non-elderly populations are lower than previous calculations had suggested.
Across 31 systematically identified national seroprevalence studies in the pre-vaccination era, the median infection fatality rate of COVID-19 was estimated to be 0.034% for people aged 0–59 years people and 0.095% for those aged 0–69 years.
The median IFR was 0.0003% at 0–19 years, 0.002% at 20–29 years, 0.011% at 30–39 years, 0.035% at 40–49 years, 0.123% at 50–59 years, and 0.506% at 60–69 years.
At a global level, pre-vaccination IFR may have been as low as 0.03% and 0.07% for 0–59 and 0–69 year old people, respectively.
These IFR estimates in non-elderly populations are lower than previous calculations had suggested.
Related review/commentary: Modeling Gone Bad., Robert W Malone MD, MS, December 30, 2022
These IFR estimates in the non-elderly population are much lower than previous calculations and models had suggested.
[...]
One scientist who clearly led this effort and led the world astray with his dire forecasting, was Neil Ferguson, PhD of Imperial College.
Ferguson’s team at Imperial College in London has claimed credit for saving millions of lives through the lockdown policies that implemented his models. It is the Imperial College models that projected millions of deaths in the first year in the UK, if stringent lockdowns were not implemented. Once implemented, Ferguson and Imperial college quickly took credit for the “success” of lockdowns.
The estimate of 3.1 million lives saved by Dr. Ferguson was derived from a Thoroughly “ludicrous unscientific exercise, whereby they purported to validate their model by using their own hypothetical projections as a counterfactual of what would happen without lockdowns.” Other models and real world data have discredited Ferguson’s models, but the damage was done. Lockdowns, quarantines, masking, poorly-tested EUA products - such as experimental vaccines have taken their toll on all of us. In the end, what, if any of them were necessary?
medrxiv.org [2022-10-21] Angelo Maria Pezzullo, Cathrine Axfors, Despina G. Contopoulos-Ioannidis, Alexandre Apostolatos, John P.A. Ioannidis, October 13, 2022 link archive General
To date, we still don’t have especially good studies on the actual causes of excess deaths by state and country when the world first went into lockdown in spring 2020.
[...]
Thus, this article reexamines data from the US CDC on all-cause excess deaths by state during peak lockdown in April 2020 using the information we now know to determine what actually caused them.
This examination concludes that, contrary to popular belief, there was no uniquely deadly strain or variant emanating out of New York in spring 2020; this is clear from the fact that several states close to New York such as Vermont, New Hampshire, and Maine experienced little to no excess deaths during that time period.
On the contrary, over 30,000 Americans appear to have been killed by mechanical ventilators or other forms of medical iatrogenesis throughout April 2020, primarily in the area around New York.
This result is not altogether surprising, as subsequent studies revealed a 97.2% mortality rate among those over age 65 who were put on mechanical ventilators in accordance with the initial guidance from the WHO—as opposed to a 26.6% mortality rate among those over age 65 who weren’t put on mechanical ventilators—before a grassroots campaign put a stop to the practice by the beginning of May 2020.
PLEASE NOTE: This implementation of the QCovid risk calculator is NOT intended for use supporting or informing clinical decision-making. It is ONLY to be used for academic research, peer review and validation purposes, and it must NOT be used with data or information relating to any individual. For full terms and conditions please see the Academic Licence. For any other use cases, please contact enquiries@innovation.ox.ac.uk quoting reference 17939.
The symptoms of COVID-19 are variable depending on the type of variant contracted, ranging from mild symptoms to critical and possibly fatal illness.[1][2] Common symptoms include coughing, fever, loss of smell (anosmia) and taste (ageusia), with less common ones including headaches, nasal congestion and runny nose, muscle pain, sore throat, diarrhea, eye irritation,[3] and toes swelling or turning purple,[4] and in moderate to severe cases breathing difficulties.[5] People with the COVID-19 infection may have different symptoms, and their symptoms may change over time. Three common clusters of symptoms have been identified: one respiratory symptom cluster with cough, sputum, shortness of breath, and fever; a musculoskeletal symptom cluster with muscle and joint pain, headache, and fatigue; a cluster of digestive symptoms with abdominal pain, vomiting, and diarrhea.[5] In people without prior ear, nose, and throat disorders, loss of taste combined with loss of smell is associated with COVID-19 and is reported in as many as 88% of symptomatic cases.[6][7][8]
Of people who show symptoms, 81% develop only mild to moderate symptoms (up to mild pneumonia), while 14% develop severe symptoms (dyspnea, hypoxia, or more than 50% lung involvement on imaging) which requiring hospitalization and 5% of patients develop critical symptoms (respiratory failure, septic shock, or multiorgan dysfunction) requiring ICU admission.[9] At least a third of the people who are infected with the virus do not develop noticeable symptoms at any point in time.[10][11] These asymptomatic carriers tend not to get tested and can still spread the disease.[11][12][13][14] Other infected people will develop symptoms later, called "pre-symptomatic", or have very mild symptoms and can also spread the virus.[14]
As is common with infections, there is a delay between the moment a person first becomes infected and the appearance of the first symptoms. The median delay for COVID-19 is four to five days[15] possibly being infectious on 1-4 of those days.[16] Most symptomatic people experience symptoms within two to seven days after exposure, and almost all will experience at least one symptom within 12 days.[15][17]
Most people recover from the acute phase of the disease. However, some people – over half of a cohort of home-isolated young adults identified in June, 2021[18][19] – continued to experience a range of effects, such as fatigue, for months even after recovery. This is the result of a condition called long COVID which can be described as a range of persistent symptoms that continue for weeks and/or months at a time.[20] Long-term damage to organs has also been observed after the onset of COVID-19. Multi-year studies are underway to further investigate the potential long-term effects of the disease.[21]
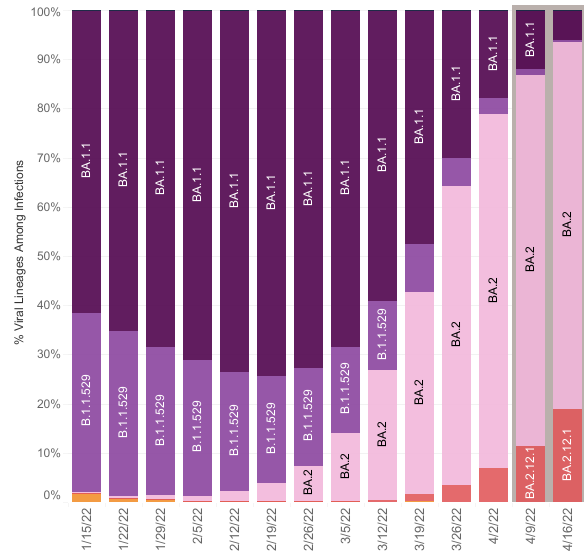
The Omicron variant became dominant in the U.S. starting in December 2021. Symptoms with the Omicron variant are less severe as they are with other variants.[22]
Most people with COVID-19 have mild illness and can recover at home. You can treat symptoms with over-the-counter medicines, such as acetaminophen (Tylenol) or ibuprofen (Motrin, Advil), to help you feel better.
[Fauci's statements to the medical community on February 28, 2020 regarding a moderate to low COVID-19 impact contradicts his more severe actions and advice to the White House.]
On the basis of a case definition requiring a diagnosis of pneumonia, the currently reported case fatality rate is approximately 2%. In another article in the Journal, Guan et al. report mortality of 1.4% among 1099 patients with laboratory-confirmed Covid-19; these patients had a wide spectrum of disease severity. If one assumes that the number of asymptomatic or minimally symptomatic cases is several times as high as the number of reported cases, the case fatality rate may be considerably less than 1%. This suggests that the overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.
nejm.org [2020-06-22] Anthony S. Fauci, M.D., H. Clifford Lane, M.D., and Robert R. Redfield, M.D., February 28, 2020 link archive General
The COVID-19 pandemic is now a major global health threat. As of 16 th March 2020, there have been 164,837 cases and 6,470 deaths confirmed worldwide. Global spread has been rapid, with 146 countries now having reported at least one case.
The last time the world responded to a global emerging disease epidemic of the scale of the current COVID-19 pandemic with no access to vaccines was the 1918-19 H1N1 influenza pandemic. In that pandemic, some communities, notably in the United States (US), responded with a variety of nonpharmaceutical interventions (NPIs) - measures intended to reduce transmission by reducing contact rates in the general population. Examples of the measures adopted during this time included closing schools, churches, bars and other social venues. Cities in which these interventions were implemented early in the epidemic were successful at reducing case numbers while the interventions remained in place and experienced lower mortality overall. However, transmission rebounded once controls were lifted.
Whilst our understanding of infectious diseases and their prevention is now very different compared to in 1918, most of the countries across the world face the same challenge today with COVID-19, a virus with comparable lethality to H1N1 influenza in 1918. Two fundamental strategies are possible:
(a) Suppression. Here the aim is to reduce the reproduction number (the average number of secondary cases each case generates), R, to below 1 and hence to reduce case numbers to low levels or (as for SARS or Ebola) eliminate human-to-human transmission. The main challenge of this approach is that NPIs (and drugs, if available) need to be maintained – at least intermittently - for as long as the virus is circulating in the human population, or until a vaccine becomes available. In the case of COVID-19, it will be at least a 12-18 months before a vaccine is available. Furthermore, there is no guarantee that initial vaccines will have high efficacy.
(b) Mitigation. Here the aim is to use NPIs (and vaccines or drugs, if available) not to interrupt transmission completely, but to reduce the health impact of an epidemic, akin to the strategy adopted by some US cities in 1918, and by the world more generally in the 1957, 1968 and 2009 influenza pandemics. In the 2009 pandemic, for instance, early supplies of vaccine were targeted at individuals with pre-existing medical conditions which put them at risk of more severe disease. In this scenario, population immunity builds up through the epidemic, leading to an eventual rapid decline in case numbers and transmission dropping to low levels.
More information on Imperial College
More information on Neil Ferguson
imperial.ac.uk (pdf doc) March 16, 2020 link archive General
After weeks of downplaying the severity of the coronavirus pandemic, why did President Trump suddenly sound so serious about it on Monday? Everyone’s best guess is that he was briefed on a new study from Imperial College in London, which estimated the death rate from the pandemic if no control measures are taken:
motherjones.com [2020-06-04] KEVIN DRUM, MARCH 17, 2020 link archive General
So how accurate has the model it been? Here are some numbers: Initially, the I-H-M-E predicted that on April 4th, the state of New York would require 65,000 hospital beds to handle infected patients. The low-end estimate was nearly 48,000 beds. In fact, on April 4, New York had fewer than 16,000 hospitalizations for Coronavirus. Many other states fell far below the model’s projections as a well.
realclearpolitics.com [2020-06-04] Ian Schwartz, April 7, 2020 link archive General
Scientist and Imperial College author Neil Ferguson said Wednesday the coronavirus death toll is unlikely to exceed 20,000 and could be much lower if lockdown measures continue, according to New Scientist. He added that he is “reasonably confident” that Britain’s health system can handle the burden of treating coronavirus patients.
washingtonexaminer.com [2020-06-04] by Andrew Mark Miller, March 26, 2020 link archive General
Our simulations are in agreement with other studies that the current epidemic wave in the UK and Italy in the absence of interventions should have an approximate duration of 2-3 months, with numbers of deaths lagging behind in time relative to overall infections. Importantly, the results we present here suggest the ongoing epidemics in the UK and Italy started at least a month before the first reported death and have already led to the accumulation of significant levels of herd immunity in both countries.
medrxiv.org Jose Lourenco, Robert Paton, Mahan Ghafari, Moritz Kraemer, Craig Thompson, Peter Simmonds, Paul Klenerman, Sunetra Gupta, March 26, 2020 link archive General
The Infection Fatality Ratio (IFR) estimates the percentage deaths in all those with an infection: the detected (cases) and those with undetected disease (asymptomatic and the not-tested group).
The IFR is used to model the estimated number of deaths in the population at large. If it's a large number approaching one percent, then the modelled outputs can report an alarming number of fatalities - providing the impetus for lockdowns.
Early in the pandemic, Imperial College London’s Report 9 modelled the impact of covid based on a publication by Verity et al. on 13 March 2000, which estimated the IFR as 0.9 percent.
This IFR gave rise to the modelled estimates ‘in an unmitigated epidemic, we would predict approximately 510,000 deaths in GB and 2.2 million in the US.’
The authors wrote this: “However, the resulting mitigated epidemic would still likely result in hundreds of thousands of deaths and health systems (most notably intensive care units) being overwhelmed many times over. For countries able to achieve it, this leaves suppression as the preferred policy option.”
A recent publication by Stanford researchers based on seroprevalence studies in the covid pre-vaccination era provides a more robust estimate of the IFR.
Across 32 studies, the median IFR of COVID-19 was estimated to be 0.035% for people aged 0-59 years and 0.095% for those aged 0-69.
We compared the two IFR estimates, which shows the Imperial College estimates are much higher than Stanfords across the age groups.
[...]
The consequences of overestimating the IFR are profound. It overpredicts the number of deaths and influences political decision-making without considering the long-term harm and well-being effects.
Overestimating the IFR is not that unusual. For example, in the Swine flu pandemic, the post-pandemic IFR was reported as 0.02%, fivefold less than the lowest estimate during the outbreak.
There are further problems with the IFR to consider. First, it assumes all deaths with a PCR positive test or covid on the death certificate were caused by SARs-CoV-2. This Is not the case, as we have shown. The IFR also doesn't account for hospital deaths or the complex interaction of multimorbidity and the assignment of causation.
An analysis distinguishing causation in under 18s, as opposed to those who died of another cause but were coincidentally infected, reported a mortality rate in < 18-year-olds of two per million—suggesting an IFR of 0.0002%, and covid is possibly the underlying cause of death in only about a quarter of young people when it is registered on the death certificate.
Invoking the precautionary principle for the widespread use of restrictions based on catastrophic predictions also underlines the misunderstanding of the basis of the principle: act only when you are sure that the benefits of your actions outweigh the negative consequences. No such evidence existed then, as lockdowns were not even contemplated in the existing pandemic plans.
trusttheevidence.substack.com [2022-10-29] Carl Heneghan, Jason Oke, Tom Jefferson, October 27, 2022 link archive General
China has finally admitted its zero-Covid approach was a total authoritarian failure by ending the experiment. Yet, an unknown event marketing agency has captured global headlines by stoking fear over ‘mass deaths’ and ‘runaway case counts.’
China is now the perfect breeding ground for new Covid variants - and Britain must act
China is likely seeing over a million COVID cases and 5,000 deaths a day, report says. But Beijing's official data is showing 7 deaths so far this week.
China COVID deaths accelerate to 9,000 a day - UK research firm Airfinity
China sees 14,700 COVID deaths every day, model suggests
Neil Ferguson
Imperial College
Airfinity
Airfinity
China risks between 1.3 and 2.1 million deaths if it ends its zero-COVID strategy
China’s COVID-19 wave forecast to have two peaks where cases could reach 4.2 million a day
Study predicts covid-19 will kill 510,000 people in Britain, 2.2 mn in US
Imperial College Predicted Catastrophe in Every Country on Earth. Then the Models Failed.
Neil Ferguson's Imperial model could be the most devastating software mistake of all time
thehighwire.com [2023-01-11] The HIGHWIRE, January 6, 2023 link archive General
Background The infection fatality rate (IFR) of Coronavirus Disease 2019 (COVID-19) varies widely according to age and residence status.
Purpose Estimate the IFR of COVID-19 in community-dwelling elderly populations and other age groups from seroprevalence studies. Study protocol: https://osf.io/47cgb.
Data Sources Seroprevalence studies done in 2020 and identified by any of four existing systematic reviews.
[...]
Conclusions The IFR of COVID-19 in community-dwelling elderly people is lower than previously reported. Very low IFRs were confirmed in the youngest populations.
[...]
medrxiv.org [2021-12-02] Cathrine Axfors, John P.A. Ioannidis, July 13, 2021 link archive General
Background: During the current worldwide pandemic, coronavirus disease 2019 (Covid-19) was first diagnosed in Iceland at the end of February. However, data are limited on how SARS-CoV-2, the virus that causes Covid-19, enters and spreads in a population.
[...]
Conclusions: In a population-based study in Iceland, children under 10 years of age and females had a lower incidence of SARS-CoV-2 infection than adolescents or adults and males. The proportion of infected persons identified through population screening did not change substantially during the screening period, which was consistent with a beneficial effect of containment efforts. (Funded by deCODE Genetics-Amgen.).
[...]
pubmed.ncbi.nlm.nih.gov [2022-11-07] Daniel F Gudbjartsson, Agnar Helgason, Hakon Jonsson, ..., Kari Stefansson, June 2020 link archive General
On Monday morning, the Centers for Disease Control and Prevention swiftly edited its Web page describing how the novel coronavirus spreads, removing recently added language saying it was “possible” that the virus spread via airborne transmission. The agency had posted information Friday suggesting the virus can transmit over a distance beyond six feet, suggesting that indoor ventilation is key to protection against its spread. Experts had been advancing that idea, and it had appeared that the agency had come around. But Monday, the CDC said an unreviewed draft had been published in error.
washingtonpost.com [2020-09-30] By Antonia Noori Farzan, Rick Noack, Lateshia Beachum, Adam Taylor, Marisa Iati, Kim Bellware, Hannah Denham, Reis Thebault and Meryl Kornfield, September 22, 2020 link archive General
Background By early April 2020, the COVID-19 pandemic had infected nearly one million people and had spread to nearly all countries worldwide. It is essential to understand where and how SARS-CoV-2 is transmitted.
Methods Case reports were extracted from the local Municipal Health Commissions of 320 prefectural cities (municipalities) in China, not including Hubei province, between 4 January and 11 February 2020. We identified all outbreaks involving three or more cases and reviewed the major characteristics of the enclosed spaces in which the outbreaks were reported and associated indoor environmental issues.
Results Three hundred and eighteen outbreaks with three or more cases were identified, involving 1245 confirmed cases in 120 prefectural cities. We divided the venues in which the outbreaks occurred into six categories: homes, transport, food, entertainment, shopping, and miscellaneous. Among the identified outbreaks, 53·8% involved three cases, 26·4% involved four cases, and only 1·6% involved ten or more cases. Home outbreaks were the dominant category (254 of 318 outbreaks; 79·9%), followed by transport (108; 34·0%; note that many outbreaks involved more than one venue category). Most home outbreaks involved three to five cases. We identified only a single outbreak in an outdoor environment, which involved two cases.
Conclusions All identified outbreaks of three or more cases occurred in an indoor environment, which confirms that sharing indoor space is a major SARS-CoV-2 infection risk.
A new study from four Chinese scientists currently awaiting peer review suggests that the coronavirus could be much more likely to spread indoors than outdoors. The proctors reviewed more than 1,000 COVID-19 cases in China, classified groups of cases into “clusters” and “outbreaks,” and summarized their findings as such:
[...]
medrxiv.org [2022-12-17] Hua Qian, Te Miao, Li Liu, Xiaohong Zheng, Danting Luo, Yuguo Li, April 07, 2020 link archive General
BACKGROUND Since its identification on the 7th of January 2020, SARS-CoV-2 has spread to more than 180 countries worldwide, causing >11,000 deaths. At present, viral disease and transmission amongst children is incompletely understood. Specifically, there is concern that children could be an important source of SARS-CoV-2 in household transmission clusters.
METHODS We performed an observational study analysing literature published between December 2019 and March 2020 of the clinical features of SARS-CoV-2 in children and descriptions of household transmission clusters of SARS-CoV-2. In these studies the index case of each cluster defined as the individual in the household cluster who first developed symptoms.
FINDINGS Drawing on studies from China, Singapore, South Korea, Japan, and Iran a broad range of clinical symptoms were observed in children. These ranged from asymptomatic to severe disease. Of the 31 household transmission clusters that were identified, 9.7% (3/31) were identified as having a paediatric index case. This is in contrast other zoonotic infections (namely H5N1 influenza virus) where 54% (30/56) of transmission clusters identified children as the index case.
INTERPRETATION Whilst SARS-CoV-2 can cause mild disease in children, the data available to date suggests that children have not played a substantive role in the intra-household transmission of SARS-CoV-2.
[...]
medrxiv.org [2022-11-18] Yanshan Zhu, Conor J. Bloxham, ..., Kirsty R Short, March 30, 2020 link archive General
Knowledge of the host response to the novel coronavirus SARS-CoV-2 remains limited, hindering the understanding of COVID-19 pathogenesis and the development of therapeutic strategies. During the course of a viral infection, host cells release exosomes and other extracellular vesicles carrying viral and host components that can modulate the immune response. The present study used a shotgun proteomic approach to map the host circulating exosomes' response to SARS-CoV-2 infection. We investigated how SARS-CoV-2 infection modulates exosome content, exosomes' involvement in disease progression, and the potential use of plasma exosomes as biomarkers of disease severity. A proteomic analysis of patient-derived exosomes identified several molecules involved in the immune response, inflammation, and activation of the coagulation and complement pathways, which are the main mechanisms of COVID-19-associated tissue damage and multiple organ dysfunctions. In addition, several potential biomarkers-such as fibrinogen, fibronectin, complement C1r subcomponent and serum amyloid P-component-were shown to have a diagnostic feature presenting an area under the curve (AUC) of almost 1. Proteins correlating with disease severity were also detected. Moreover, for the first time, we identified the presence of SARS-CoV-2 RNA in the exosomal cargo, which suggests that the virus might use the endocytosis route to spread infection. Our findings indicate circulating exosomes' significant contribution to several processes-such as inflammation, coagulation, and immunomodulation-during SARS-CoV-2 infection. The study's data are available via ProteomeXchange with the identifier PXD021144.
pubmed.ncbi.nlm.nih.gov [2023-01-09] Elettra Barberis, Virginia V Vanella, ..., Marcello Manfredi, February 2021 link archive General
Public health officials attempting to contain the new coronavirus are trying to figure out how easily it spreads. One key question is whether people who are infected but show no symptoms can infect other people.
"If you have a lot of people who [have mild disease or are] asymptomatic and not seeking medical care for respiratory illness but are still contagious, you're going to have a very difficult time," says Jeffrey Shaman, a professor of environmental health sciences at Columbia University.
Two previous deadly outbreaks of coronavirus – SARS and MERS – only spread from people who were showing symptoms of disease.
But Shaman has looked at more common coronaviruses, in particular four other coronaviruses that usually don't cause anything more serious than a cold. He's found many people shed those viruses even when they report no symptoms at all. (His results are not peer-reviewed but are available as a preprint).
His study found the coronavirus in the nasal passages of people who didn't report any symptoms, "and it's going to leak out as they're speaking and breathing and coughing and sneezing and wiping their nose," Shaman says. "Whether it's ... a sufficient quantity to make somebody else infectious, we can't discern that from what we've done."
Likewise, it's hard to know what's up with the novel coronavirus. Scientists in Germany reported a case in theNew England Journal of Medicine on Jan. 30 in which a visitor from China without symptoms passed the disease along to a colleague in Munich. But, as Science magazine first reported, that was wrong. The woman actually did have symptoms.
[...]
wbur.org [2022-11-24] Richard Harris, February 05, 2020 link archive General
As the coronavirus landed in the U.S. in January, scientists began whispering about an apparent difference from its notorious sibling, the virus that caused SARS: People infected with this one could easily infect others — even if they had no symptoms.
The first reports seemed questionable, and many infectious disease experts didn’t believe them. Two months later, the virus has swarmed across the United States, forcing tens of millions into self-isolation. And now some experts believe that asymptomatic transmission — the passing of a virus from an infected person who feels just fine to others — is driving the pandemic.
Concerns about people without symptoms infecting others were part of the reason county health officers across California, including most of the Bay Area, this week began advising everyone to wear face coverings in public, whether they feel sick or not. The Centers for Disease Control and Prevention issued a nationwide advisory on Friday.
[...]
sfchronicle.com [2022-11-23] Erin Allday, April 3, 2020 link archive General
8 JUN 2020: Maria Van Kerkhove, head of the World Health Organization’s emerging diseases and zoonosis unit, says transmission of the coronavirus by people who aren’t showing symptoms is "very rare.” She spoke Monday at a briefing in Geneva.
She has just contradicted everything we´ve been hearing for the last four months! She´s destroyed the justification for masks and societal lockdown. Isolation of symptomatic cases (a quarantine) is what should’ve happened from the very beginning. No masks. No social distancing. No lockdowns. Just a good old fashioned quarantine of sick individuals. Not a complete destruction of the world economy causing ripples of closed businesses, unbelievable unemployment, an increasing suicide rate, and general mass fear throughout the world. Shame on these people..This announcement, comes, RIGHT at the moment of the protests and rioting in the US, “it’s ok to go outside guys”.
9 JUN 2020: Harvard Global Health Institute: “The WHO created confusion yesterday when it reported that asymptomatic patients rarely spread the disease,” an email from the Harvard Global Health Institute said Tuesday. “All of the best evidence suggests that people without symptoms can and do readily spread SARS-CoV-2, the virus that causes Covid-19. (Source)
The misplaced idea that asymptomatic Covid cases drove viral spread, was the cornerstone of public health authorities enacting draconian mandates and highly destructive lockdowns. Now, data from a new study covering 42 countries shows people with asymptomatic Covid infections are 68% less likely to pass the virus on, highlighting another failure of public health authorities.
... not novel... no pandemic.. no variants... campaign of coercion & terror to address a stated objective. Dr David Martin, SG!! Who can tell us what the Vaxxed can do about this synthetic recombinant chimera protein? "There was no novel Coronavirus. Check of gene sequence vs all patent records showed not novel since 1999!
There are 120 patented pieces of evidence showing total fallacy of claim 'novel'!
More information on Coronavirus patents & David Martin
More information on Peter Daszak (of EcoHealth Alliance)
More information on Ralph Baric at UNC-Chapel Hill
["A Novel Bat Coronavirus Closely Related to SARS-CoV-2 Contains Natural Insertions at the S1/S2 Cleavage Site of the Spike Protein" - US National Library of Medicine, May 11, 2020.]
["SARS-like WIV1-CoV poised for human emergence" - PNAS, March 15, 2016.]
More information on WHO Global Preparedness Monitoring Board
odysee.com [2021-07-23] @Jadu200 channel, July 10, 2021 link archive General
A helper cell for producing an infectious, replication defective, coronavirus (or more generally nidovirus) particle cell comprises (a) a nidovirus permissive cell; (b) a nidovirus replicon RNA comprising the nidovirus packaging signal and a heterologous RNA sequence, wherein the replicon RNA further lacks a sequence encoding at least one nidovirus structural protein; and (c) at least one separate helper RNA encoding the at least one structural protein absent from the replicon RNA, the helper RNA(s) lacking the nidovirus packaging signal. The combined expression of the replicon RNA and the helper RNA in the nidovirus permissive cell produces an assembled nidovirus particle which comprises the heterologous RNA sequence, is able to infect a cell, and is unable to complete viral replication in the absence of the helper RNA due to the absence of the structural protein coding sequence in the packaged replicon. Compositions for use in making such helper cells, along with viral particles produced from such cells, compositions of such viral particles, and methods of making and using such viral particles, are also disclosed.
patents.google.com [2021-07-24] Application filed by University of North Carolina at Chapel Hill: 2002-04-19, Application granted: 2007-10-09 link archive General
The present invention provides a live, attenuated coronavirus comprising a variant replicase gene encoding polyproteins comprising a mutation in one or more of non-structural protein(s) (nsp)-10, nsp-14, nsp-15 or nsp-16. The coronavirus may be used as a vaccine for treating and/or preventing a disease, such as infectious bronchitis, in a subject.
Gammacoronavirus is a genus of animal virus belonging to the family Coronaviridae. Coronaviruses are enveloped viruses with a positive-sense single-stranded RNA genome and a helical symmetry.
[...]
Coronaviruses primarily infect the upper respiratory or gastrointestinal tract of mammals and birds. Five to six different currently known strains of coronaviruses infect humans. The most publicized human coronavirus, SARS-CoV which causes severe acute respiratory syndrome (SARS), has a unique pathogenesis because it causes both upper and lower respiratory tract infections and can also cause gastroenteritis. Middle East respiratory syndrome coronavirus (MERS-CoV) also causes a lower respiratory tract infection in humans. Coronaviruses are believed to cause a significant percentage of all common colds in human adults.
[...]
The variant replicase gene of the coronavirus of the present invention may be derived from an alphacoronavirus such as TGEV; a betacoronavirus such as MHV; or a gammacoronavirus such as IBV.
As used herein the term “derived from” means that the replicase gene comprises substantially the same nucleotide sequence as the wild-type replicase gene of the relevant coronavirus. For example, the variant replicase gene of the present invention may have up to 80%, 85%, 90%, 95%, 98% or 99% identity with the wild type replicase sequence. The variant coronavirus replicase gene encodes a protein comprising a mutation in one or more of non-structural protein (nsp)-10, nsp-14, nsp-15 or nsp-16 when compared to the wild-type sequence of the non-structural protein.
[...]
The virus isolated from the Dutch cases was identified by the Dutch Research Institute at Deventer as a new strain that they called D388. The Chinese connection came from further tests which showed that the virus was 99% similar to the Chinese QX viruses. A live attenuated QX-like IBV vaccine strain has now been developed.
IBV is an enveloped virus that replicates in the cell cytoplasm and contains an non-segmented, single-stranded, positive sense RNA genome. IBV has a 27.6 kb RNA genome and like all coronaviruses contains the four structural proteins; spike glycoprotein (S), small membrane protein (E), integral membrane protein (M) and nucleocapsid protein (N) which interacts with the genomic RNA.
The genome is organised in the following manner: 5′UTR—polymerase (replicase) gene—structural protein genes (S-E-M-N)—UTR 3′; where the UTR are untranslated regions (each ˜500 nucleotides in IBV).
[...]
More information on Pirbright Institute
patents.google.com [2021-07-23] Filed on: 2015-07-23, Granted: 2018-11-20 link archive General
Disclosed herein is a newly isolated human coronavirus (SARS-CoV), the causative agent of severe acute respiratory syndrome (SARS). Also provided are the nucleic acid sequence of the SARS-CoV genome and the amino acid sequences of the SARS-CoV open reading frames, as well as methods of using these molecules to detect a SARS-CoV and detect infections therewith. Immune stimulatory compositions are also provided, along with methods of their use.
patents.google.com [2021-07-25] Application filed by Centers of Disease Control and Prevention CDC: 2004-04-12, Application granted: 2007-05-22 link archive General
Disclosed herein is a newly isolated human coronavirus (SARS-CoV), the causative agent of severe acute respiratory syndrome (SARS). Also provided are the nucleic acid sequence of the SARS-CoV genome and the amino acid sequences of the SARS-CoV open reading frames, as well as methods of using these molecules to detect a SARS-CoV and detect infections therewith. Immune stimulatory compositions are also provided, along with methods of their use.
[...]
patents.google.com [2021-07-25] Application filed by Centers of Disease Control and Prevention CDC: 2007-05-14, Application granted: 2010-08-17 link archive General
The invention provides compositions and methods that are useful for preventing and treating a coronavirus infection in a subject. More specifically, the invention provides peptides and conjugates and pharmaceutical compositions containing those peptides and conjugates that block fusion of a coronavirus, such as the SARS virus, to a target cell. This blocking mechanism prevents or treats a coronavirus infection, such as a SARS infection, in a subject, such as a human subject.
The present invention relates in part to amino acid sequences that are directed against and/or that can specifically bind to an envelope protein of a virus, as well as to compounds or constructs, and in particular proteins and polypeptides, that comprise or essentially consist of one or more such amino acid sequences.
An outbreak of a virulent respiratory virus, now known as Severe Acute Respiratory Syndrome (SARS), was identified in Hong Kong, China and a growing number of countries around the world in 2003. The invention relates to nucleic acids and proteins from the SARS coronavirus. These nucleic acids and proteins can be used in the preparation and manufacture of vaccine formulations, diagnostic reagents, kits, etc. The invention also provides methods for treating SARS by administering small molecule antiviral compounds, as well as methods of identifying potent small molecules for the treatment of SARS.
The invention relates to the spike protein from the virus (SARS-CoV) that is etiologically linked to severe acute respiratory syndrome (SARS); polypeptides and peptide fragments of the spike protein; nucleic acid segments and constructs that encode the spike protein, polypeptides and peptide fragments of the spike protein, and coupled proteins that include the spike protein or a portion thereof; peptidomimetics; vaccines; methods for vaccination and treatment of severe acute respiratory syndrome; antibodies; aptamers; and kits containing immunological compositions, or antibodies (or aptamers) that bind to the spike protein.
Assigned to: US Department of Health and Human Services
Status: Abandoned
patents.google.com [2021-07-23] Application filed by US Department of Health and Human Services: 2006-01-19, Assigned to: HEALTH AND HUMAN SERVICES; GOVERNMENT OF UNITED STATES OF AMERICA: 2006-05-03 link archive General
A list of patents linked to specific diseases and viruses is being shared with the suggestion that it is proof that viruses are manmade. This is false, and a misinterpretation of the types of patent listed.
[...]
reuters.com [2022-04-27] OCTOBER 27, 2020 link archive General
Emerging infectious diseases, such as severe acute respiratory syndrome (SARS) and Zika virus disease, present a major threat to public health1–3. Despite intense research efforts, how, when and where new diseases appear are still a source of considerable uncertainty. A severe respiratory disease was recently reported in Wuhan, Hubei province, China. As of 25 January 2020, at least 1,975 cases had been reported since the first patient was hospitalized on 12 December 2019. Epidemiological investigations have suggested that the outbreak was associated with a seafood market in Wuhan. Here we study a single patient who was a worker at the market and who was admitted to the Central Hospital of Wuhan on 26 December 2019 while experiencing a severe respiratory syndrome that included fever, dizziness and a cough. Metagenomic RNA sequencing4 of a sample of bronchoalveolar lavage fluid from the patient identified a new RNA virus strain from the family Coronaviridae, which is designated here ‘WH-Human 1’ coronavirus (and has also been referred to as ‘2019-nCoV’). Phylogenetic analysis of the complete viral genome (29,903 nucleotides) revealed that the virus was most closely related (89.1% nucleotide similarity) to a group of SARS-like coronaviruses (genus Betacoronavirus, subgenus Sarbecovirus) that had previously been found in bats in China5. This outbreak highlights the ongoing ability of viral spill-over from animals to cause severe disease in humans.
ncbi.nlm.nih.gov [2023-05-05] Fan Wu, Su Zhao, ..., Edward C. Holmes, Yong-Zhen Zhang, February 2020 link archive General
BLAST finds regions of similarity between biological sequences. The program compares nucleotide or protein sequences to sequence databases and calculates the statistical significance.
In early 2020, a few months after the Covid-19 pandemic began, scientists were able to sequence the full genome of SARS-CoV-2, the virus that causes the Covid-19 infection. While many of its genes were already known at that point, the full complement of protein-coding genes was unresolved.
Now, after performing an extensive comparative genomics study, MIT researchers have generated what they describe as the most accurate and complete gene annotation of the SARS-CoV-2 genome. In their study, which appears today in Nature Communications, they confirmed several protein-coding genes and found that a few others that had been suggested as genes do not code for any proteins.
“We were able to use this powerful comparative genomics approach for evolutionary signatures to discover the true functional protein-coding content of this enormously important genome,” says Manolis Kellis, who is the senior author of the study and a professor of computer science in MIT’s Computer Science and Artificial Intelligence Laboratory (CSAIL) as well as a member of the Broad Institute of MIT and Harvard.
news.mit.edu [2021-07-02] Anne Trafton, May 11, 2021 link archive General
Biologists from the Applied Physics Lab work to track the mutation of SARS-CoV-2, the virus that causes COVID-19
[...]
"When this virus was first sequenced in China, that information was helpful in starting the process to develop a vaccine," Thielen explained. "What we're doing informs whether or not the virus is mutating away from that original sequence, and how quickly. Based on the mutation rate, early data indicates that this would likely be a single vaccine rather than one that needs to be updated each year, like the flu shot."
hub.jhu.edu [2021-07-02] Amanda Zrebiec, Mar 30, 2020 link archive General
What is genomic sequencing and why is it important to understand the genomic sequence of COVID-19?
Thielen: Genomic sequencing is a technique that allows us to read and interpret genetic information found within DNA or RNA. When we look at virus genome sequences from patient samples that test positive for COVID-19, we're interested in understanding where their version of the virus originated. For example, does the virus look similar to how it looks in Washington State? Or in New York? Or in Europe? Right now, we're working to analyze many genome sequences from SARS-CoV-2, the virus that causes COVID-19, that are circulating in the Baltimore area and in Maryland. Our goal is to understand how the virus is evolving as it spreads. So far, there are over 1,000 COVID-19 genomes that have been published worldwide.
A loading buffer is injected into a hand-held DNA sequencer to prepare it for operation. CREDIT:JOHNS HOPKINS APL
Governments around the world will need to invest billions of euros more in coronavirus vaccine development, to take forward some promising candidates that are emerging, the Coalition for Epidemic Preparedness Innovations (CEPI) said on Friday.
[...]
Researchers sprang into action once the genome sequence of COVID-19 was published online in mid-January, and the global quest for a vaccine includes 10 and 15 serious programmes. CEPI is funding six of these, including projects with the German company CureVac and the US companies Inovio Pharmaceuticals and Moderna, as well as the universities of Oxford, Imperial College London, and Queensland in Australia.
sciencebusiness.net [2021-03-05] By Éanna Kelly, 13 Mar 2020 link archive General
A guide to implementation for maximum impact on public health
[...]
5.1.1 Identifying the causative agent of COVID-19
SARS-CoV-2 was independently identified and sequenced in early 2020 by Wu et al., Lu et al. and Zhou et al. (52, 59,60). Several different metagenomic next-generation sequencing (mNGS) approaches were used to identify the causative pathogen of COVID-19. Metagenomic sequencing permits untargeted sequencing of nucleic acid in a sample, and can therefore identify viral RNA or DNA if present at high enough copy numbers relative to DNA or RNA from other sources (see also section 6.5.1). Completion of the full-length virus genome sequences, including the genome termini, generally involved Sanger sequencing and a 5’/3’ rapid amplification of cDNA ends (RACE) method. This method is cost-efficient for sequencing short regions of a genome that may be missed with metagenomic methods, but relies on previous knowledge of the sequence information relatively close to the missing region.
[...]
5.2.1 Host receptor usage
Since viruses can replicate only inside the living cells of a host organism, determining the host cellular receptor used by SARS-CoV-2 is essential to understanding its basic biology. Receptor binding is mediated by the S protein of the virus. Genetic similarities in the S protein receptorbinding motif between SARS-CoV-2 and other, previously investigated coronaviruses have helped to identify the cellular receptor to which SARS-CoV-2 binds, and hence the cell types that it might infect. Initial studies indicated that SARS-CoV-2 was likely to use the same angiotensin-converting enzyme 2 (ACE2) cell receptor as the 2002–2003 SARS-CoV, and was likely to bind to this receptor with high affinity (70, 71). Most amino acid residues that are known to be essential for ACE2 binding by SARS-CoV are conserved in SARS-CoV-2 (70). In vitro assays confirm the strong specificity for ACE2 suggested by direct structural studies (72).
apps.who.int [2021-07-02] (pdf doc) 8 January 2021 link archive General
Programmed ribosomal frameshifting is an essential mechanism used for the expression of orf1b in coronaviruses. Comparative analysis of the frameshift region reveals a universal shift site U_UUA_AAC, followed by a predicted downstream RNA structure in the form of either a pseudoknot or kissing stem loops. Frameshifting in SARS-CoV has been characterized in cultured mammalian cells using a dual luciferase reporter system and mass spectrometry. Mutagenic analysis of the SARS-CoV shift site and mass spectrometry of an affinity tagged frameshift product confirmed tandem tRNA slippage on the sequence U_UUA_AAC. Analysis of the downstream pseudoknot stimulator of frameshifting in SARS-CoV shows that a proposed RNA secondary structure in loop II and two unpaired nucleotides at the stem I-stem II junction in SARS-CoV are important for frameshift stimulation. These results demonstrate key sequences required for efficient frameshifting, and the utility of mass spectrometry to study ribosomal frameshifting.
pubmed.ncbi.nlm.nih.gov [2021-07-11] Pavel V Baranov 1, Clark M Henderson, Christine B Anderson, Raymond F Gesteland, John F Atkins, Michael T Howard, Feb 20, 2005 link archive General
Studies have demonstrated that ~60%–80% of emerging infectious diseases (EIDs) in humans originated from wild life. Bats are natural reservoirs of a large variety of viruses, including many important zoonotic viruses that cause severe diseases in humans and domestic animals. However, the understanding of the viral population and the ecological diversity residing in bat populations is unclear, which complicates the determination of the origins of certain EIDs. Here, using bats as a typical wildlife reservoir model, virome analysis was conducted based on pharyngeal and anal swab samples of 4440 bat individuals of 40 major bat species throughout China. The purpose of this study was to survey the ecological and biological diversities of viruses residing in these bat species, to investigate the presence of potential bat-borne zoonotic viruses and to evaluate the impacts of these viruses on public health. The data obtained in this study revealed an overview of the viral community present in these bat samples. Many novel bat viruses were reported for the first time and some bat viruses closely related to known human or animal pathogens were identified. This genetic evidence provides new clues in the search for the origin or evolution pattern of certain viruses, such as coronaviruses and noroviruses. These data offer meaningful ecological information for predicting and tracing wildlife-originated EIDs.
ncbi.nlm.nih.gov [2021-07-25] Zhiqiang Wu, Li Yang, Xianwen Ren, Guimei He, Junpeng Zhang, Jian Yang, Zhaohui Qian, Jie Dong, Lilian Sun, Yafang Zhu, Jiang Du Fan Yang, Shuyi Zhang, and Qi Jin, Aug 11, 2015 link archive General
- ACE2 Receptor / Spike Protein -
More information on spike proteins and ACE2 receptors at Coronavirus Vaccines
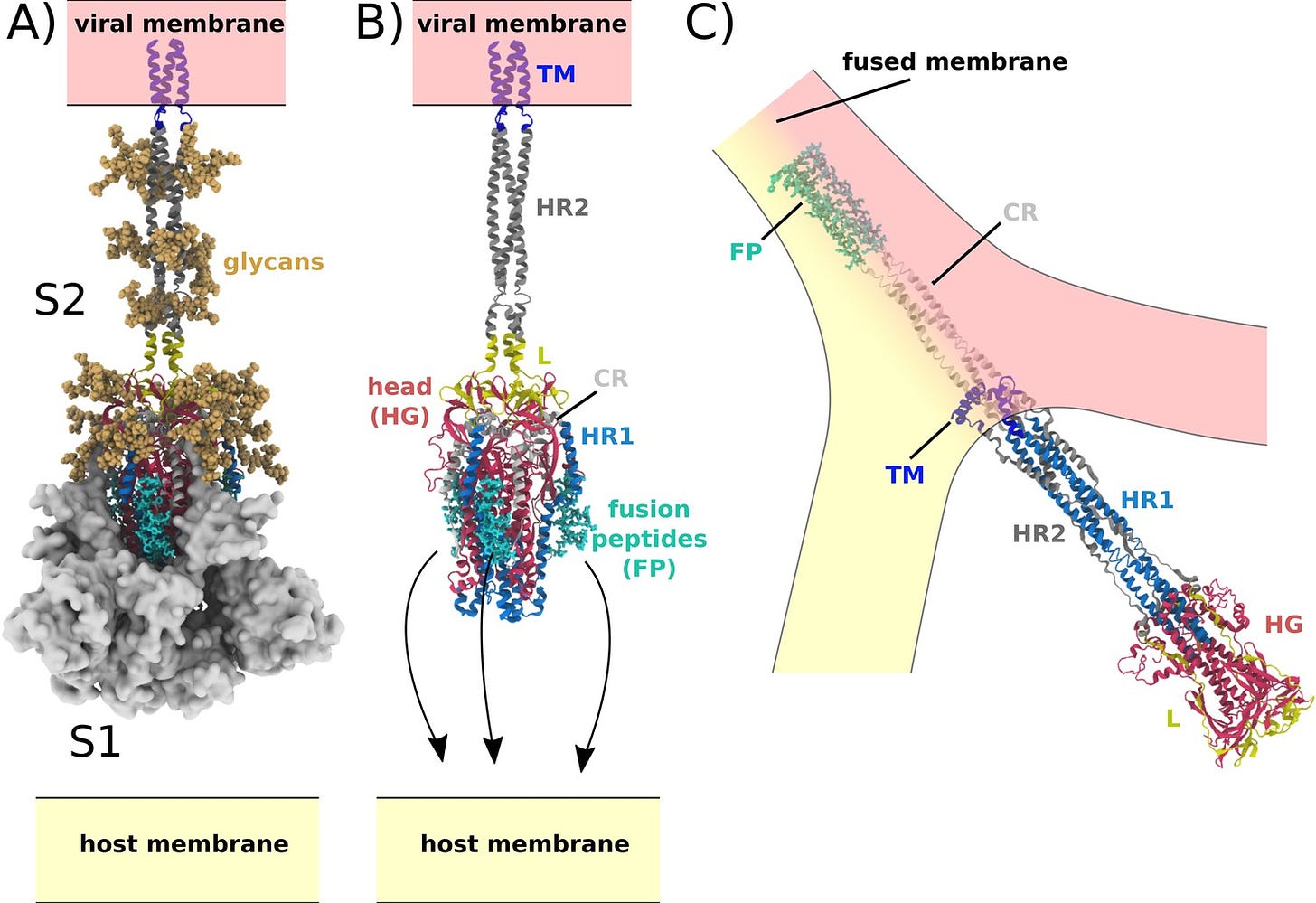
The spike glycoprotein of the newly emerged SARS-CoV-2 contains a potential cleavage site for furin proteases. This observation has implications for the zoonotic origin of the virus and its epidemic spread in China.
The membrane of coronaviruses harbors a trimeric transmembrane spike (S) glycoprotein (pictured) which is essential for entry of virus particles into the cell. The S protein contains two functional domains: a receptor binding domain, and a second domain which contains sequences that mediate fusion of the viral and cell membranes. The S glycoprotein must be cleaved by cell proteases to enable exposure of the fusion sequences and hence is needed for cell entry.
The nature of the cell protease that cleaves the S glycoprotein varies according to the coronavirus. The MERS-CoV S glycoprotein contains a furin cleavage site and is probably processed by these intracellular proteases during exit from the cell. The virus particles are therefore ready for entry into the next cell. In contrast, the SARS-CoV S glycoprotein is uncleaved upon virus release from cells; it is likely cleaved during virus entry into a cell.
Proteolytic cleavage of the S glycoprotein can determine whether the virus can cross species, e.g. from bats to humans. For example, the S glycoprotein from a MERS-like CoV from Ugandan bats can bind to human cells but cannot mediate virus entry. However, if the protease trypsin is included during infection, the S glycoprotein is cleaved and virus entry takes place. This observation demonstrates that cleavage of the S glycoprotein is a barrier to zoonotic coronavirus transmission.
[...]
virology.ws [2022-01-21] February 13, 2020 link archive General
The unprecedented pandemic of pneumonia caused by a novel coronavirus, SARS-CoV-2, in China and beyond has had major public health impacts on a global scale [1, 2]. Although bats are regarded as the most likely natural hosts for SARS-CoV-2 [3], the origins of the virus remain unclear. Here, we report a novel bat-derived coronavirus, denoted RmYN02, identified from a metagenomic analysis of samples from 227 bats collected from Yunnan Province in China between May and October 2019. Notably, RmYN02 shares 93.3% nucleotide identity with SARS-CoV-2 at the scale of the complete virus genome and 97.2% identity in the 1ab gene, in which it is the closest relative of SARS-CoV-2 reported to date. In contrast, RmYN02 showed low sequence identity (61.3%) to SARS-CoV-2 in the receptor-binding domain (RBD) and might not bind to angiotensin-converting enzyme 2 (ACE2). Critically, and in a similar manner to SARS-CoV-2, RmYN02 was characterized by the insertion of multiple amino acids at the junction site of the S1 and S2 subunits of the spike (S) protein. This provides strong evidence that such insertion events can occur naturally in animal betacoronaviruses.
ncbi.nlm.nih.gov [2021-07-25] Hong Zhou, Xing Chen, Tao Hu, Juan Li, Hao Song, Yanran Liu, Peihan Wang, Di Liu, Jing Yang, Edward C. Holmes, Alice C. Hughes, Yuhai Bi, and Weifeng Shi, May 11, 2020 link archive General
SARS-CoV-2 has resulted in a global pandemic and shutdown economies around the world. Sequence analysis indicates that the novel coronavirus (CoV) has an insertion of a furin cleavage site (PRRAR) in its spike protein. Absent in other group 2B CoVs, the insertion may be a key factor in the replication and virulence of SARS-CoV-2. To explore this question, we generated a SARS-CoV-2 mutant lacking the furin cleavage site (ΔPRRA) in the spike protein. This mutant virus replicated with faster kinetics and improved fitness in Vero E6 cells. The mutant virus also had reduced spike protein processing as compared to wild-type SARS-CoV-2. In contrast, the ΔPRRA had reduced replication in Calu3 cells, a human respiratory cell line, and had attenuated disease in a hamster pathogenesis model. Despite the reduced disease, the ΔPRRA mutant offered robust protection from SARS-CoV-2 rechallenge. Importantly, plaque reduction neutralization tests (PRNT 50 ) with COVID-19 patient sera and monoclonal antibodies against the receptor-binding domain found a shift, with the mutant virus resulting in consistently reduced PRNT 50 titers. Together, these results demonstrate a critical role for the furin cleavage site insertion in SARS-CoV-2 replication and pathogenesis. In addition, these findings illustrate the importance of this insertion in evaluating neutralization and other downstream SARS-CoV-2 assays.
Importance: As COVID-19 has impacted the world, understanding how SARS-CoV-2 replicates and causes virulence offers potential pathways to disrupt its disease. By removing the furin cleavage site, we demonstrate the importance of this insertion to SARS-CoV-2 replication and pathogenesis. In addition, the findings with Vero cells indicate the likelihood of cell culture adaptations in virus stocks that can influence reagent generation and interpretation of a wide range of data including neutralization and drug efficacy. Overall, our work highlights the importance of this key motif in SARS-CoV-2 infection and pathogenesis.
Article summary: A deletion of the furin cleavage site in SARS-CoV-2 amplifies replication in Vero cells, but attenuates replication in respiratory cells and pathogenesis in vivo. Loss of the furin site also reduces susceptibility to neutralization in vitro .
pubmed.ncbi.nlm.nih.gov [2022-12-14] Bryan A Johnson, Xuping Xie, ..., Vineet D Menachery, Aug 2020 link archive General
LA JOLLA—Scientists have known for a while that SARS-CoV-2’s distinctive “spike” proteins help the virus infect its host by latching on to healthy cells. Now, a major new study shows that the virus spike proteins (which behave very differently than those safely encoded by vaccines) also play a key role in the disease itself.
The paper, published on April 30, 2021, in Circulation Research, also shows conclusively that COVID-19 is a vascular disease, demonstrating exactly how the SARS-CoV-2 virus damages and attacks the vascular system on a cellular level. The findings help explain COVID-19’s wide variety of seemingly unconnected complications, and could open the door for new research into more effective therapies.
“A lot of people think of it as a respiratory disease, but it’s really a vascular disease,” says Assistant Research Professor Uri Manor, who is co-senior author of the study. “That could explain why some people have strokes, and why some people have issues in other parts of the body. The commonality between them is that they all have vascular underpinnings.”
The following article was published by Salk Institute on April 30, 2021. It reports on a study funded by a number of health organizations, including the National Institutes of Health which discovered that SARS-CoV-2 is in fact a vascular disease, not a respiratory disease.
According to the study, the SARS-CoV-2’s spike protein damages and attacks the vascular system on a cellular level. The researchers believe that explains the wide variety of seemingly unconnected complications related to COVID-19.
Taking the study deeper, the researchers created a “pseudovirus” that was surrounded by SARS-CoV-2 classic crown of spike proteins, but did not contain the actual virus. They found that “exposure to this pseudovirus resulted in damage to the lungs and arteries of an animal model – proving that the spike protein alone was enough to cause the disease”.
[...]
covidcalltohumanity.org [2021-08-01] June 10, 2021 link archive General
May 31, 2021 (LifeSiteNews) — New research shows that the coronavirus spike protein from COVID-19 vaccination unexpectedly enters the bloodstream, which is a plausible explanation for thousands of reported side-effects from blood clots and heart disease to brain damage and reproductive issues, a Canadian cancer vaccine researcher said last week.
“We made a big mistake. We didn’t realize it until now,” said Byram Bridle, a viral immunologist and associate professor at University of Guelph, Ontario, in an interview with Alex Pierson last Thursday, in which he warned listeners that his message was “scary.”
“We thought the spike protein was a great target antigen, we never knew the spike protein itself was a toxin and was a pathogenic protein. So by vaccinating people we are inadvertently inoculating them with a toxin,” Bridle said on the show, which is not easily found in a Google search but went viral on the internet this weekend.
[...]
More information on Byram Bridle
lifesitenews.com [2021-08-01] Celeste McGovern, May 31, 2021 link archive General
Antibodies against the receptor-binding domain (RBD) of the SARS-CoV-2 spike protein prevent SARS-CoV-2 infection. However, the effects of antibodies against other spike protein domains are largely unknown. Here, we screened a series of anti-spike monoclonal antibodies from coronavirus disease 2019 (COVID-19) patients and found that some of antibodies against the N-terminal domain (NTD) induced the open conformation of RBD and thus enhanced the binding capacity of the spike protein to ACE2 and infectivity of SARS-CoV-2. Mutational analysis revealed that all of the infectivity-enhancing antibodies recognized a specific site on the NTD. Structural analysis demonstrated that all infectivity-enhancing antibodies bound to NTD in a similar manner. The antibodies against this infectivity-enhancing site were detected at high levels in severe patients. Moreover, we identified antibodies against the infectivity-enhancing site in uninfected donors, albeit at a lower frequency. These findings demonstrate that not only neutralizing antibodies but also enhancing antibodies are produced during SARS-CoV-2 infection.
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) causes a broad range of clinical responses including prominent microvascular damage. The capacity of SARS-CoV-2 to infect vascular cells is still debated. Additionally, the SARS-CoV-2 Spike (S) protein may act as a ligand to induce non-infective cellular stress. We tested this hypothesis in pericytes (PCs), which are reportedly reduced in the heart of patients with severe coronavirus disease-2019 (COVID-19). Here we newly show that the in vitro exposure of primary human cardiac PCs to the SARS-CoV-2 wildtype strain or the α and δ variants caused rare infection events. Exposure to the recombinant S protein alone elicited signalling and functional alterations, including: (1) increased migration, (2) reduced ability to support endothelial cell (EC) network formation on Matrigel, (3) secretion of pro-inflammatory molecules typically involved in the cytokine storm, and (4) production of pro-apoptotic factors causing EC death. Next, adopting a blocking strategy against the S protein receptors angiotensin-converting enzyme 2 (ACE2) and CD147, we discovered that the S protein stimulates the phosphorylation/activation of the extracellular signal-regulated kinase 1/2 (ERK1/2) through the CD147 receptor, but not ACE2, in PCs. The neutralisation of CD147, either using a blocking antibody or mRNA silencing, reduced ERK1/2 activation, and rescued PC function in the presence of the S protein. Immunoreactive S protein was detected in the peripheral blood of infected patients. In conclusion, our findings suggest that the S protein may prompt PC dysfunction, potentially contributing to microvascular injury. This mechanism may have clinical and therapeutic implications.
portlandpress.com [2022-11-22] Elisa Avolio, Michele Carrabba, ..., Paolo Madeddu, DECEMBER 15 2021 link archive General
Acute lung injury (ALI) leading to acute respiratory distress syndrome is the major cause of COVID-19 lethality. Cell entry of SARS-CoV-2 occurs via the interaction between its surface spike protein (SP) and angiotensin-converting enzyme-2 (ACE2). It is unknown if the viral spike protein alone is capable of altering lung vascular permeability in the lungs or producing lung injury in vivo. To that end, we intratracheally instilled the S1 subunit of SARS-CoV-2 spike protein (S1SP) in K18-hACE2 transgenic mice that overexpress human ACE2 and examined signs of COVID-19-associated lung injury 72 h later. Controls included K18-hACE2 mice that received saline or the intact SP and wild-type (WT) mice that received S1SP. K18-hACE2 mice instilled with S1SP exhibited a decline in body weight, dramatically increased white blood cells and protein concentrations in bronchoalveolar lavage fluid (BALF), upregulation of multiple inflammatory cytokines in BALF and serum, histological evidence of lung injury, and activation of signal transducer and activator of transcription 3 (STAT3) and nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) pathways in the lung. K18-hACE2 mice that received either saline or SP exhibited little or no evidence of lung injury. WT mice that received S1SP exhibited a milder form of COVID-19 symptoms, compared with the K18-hACE2 mice. Furthermore, S1SP, but not SP, decreased cultured human pulmonary microvascular transendothelial resistance (TER) and barrier function. This is the first demonstration of a COVID-19-like response by an essential virus-encoded protein by SARS-CoV-2 in vivo. This model of COVID-19-induced ALI may assist in the investigation of new therapeutic approaches for the management of COVID-19 and other coronaviruses.
pubmed.ncbi.nlm.nih.gov [2022-12-31] Ruben M L Colunga Biancatelli, Pavel A Solopov, ..., Paul E Marik, John D Catravas, August 2021 link archive General
Human prion protein and prion-like protein misfolding are widely recognized as playing a causal role in many neurodegenerative diseases. Based on in vitro and in vivo experimental evidence relating to prion and prion-like disease, we extrapolate from the compelling evidence that the spike glycoprotein of SARS-CoV-2 contains extended amino acid sequences characteristic of a prion-like protein to infer its potential to cause neurodegenerative disease. We propose that vaccine-induced spike protein synthesis can facilitate the accumulation of toxic prion-like fibrils in neurons. We outline various pathways through which these proteins could be expected to distribute throughout the body. We review both cellular pathologies and the expression of disease that could become more frequent in those who have undergone mRNA vaccination. Specifically, we describe the spike protein’s contributions, via its prion-like properties, to neuroinflammation and neurodegenerative diseases; to clotting disorders within the vasculature; to further disease risk due to suppressed prion protein regulation in the context of widely prevalent insulin resistance; and to other health complications. We explain why these prion-like characteristics are more relevant to vaccine-related mRNA-induced spike proteins than natural infection with SARS-CoV-2. We note with an optimism an apparent loss of prion-like properties among the current Omicron variants. We acknowledge that the chain of pathological events described throughout this paper is only hypothetical and not yet verified. We also acknowledge that the evidence we usher in, while grounded in the research literature, is currently largely circumstantial, not direct. Finally, we describe the implications of our findings for the general public, and we briefly discuss public health recommendations we feel need urgent consideration.
An earlier version of this article was previously posted to the Authorea preprint server on August 16, 2022.
The COVIDD-19 vaccination campaign was launched in late 2020 with no assurances on long-term safety and full liability protection to those involved with mass vaccination via the PREP Act and the National Childhood Vaccine Injury Act of 1986. There is now abundant evidence that the synthetic lipid nanoparticles travel into the brain and install the genetic code (mRNA or adenoviral DNA) for the SARS-CoV-2 Spike protein. As this protein is produced and accumulates in the brain, it can cause inflammation and also fold into an amyloid plaque. Thus, there is strong rationale for some vaccine recipients to develop mild cognitive dysfunction, Alzheimer’s like dementia, and other forms of neurocognitive decline. Because seniors were heavily vaccinated, many families and doctors will attribute clinical changes to advanced age and not the vaccine. They should understand in each and every case, that COVID-19 vaccination should be considered a determinant of cognitive decline in a previously healthy person.
ncbi.nlm.nih.gov [2023-02-19] Stephanie Seneff, Anthony M Kyriakopoulos, Greg Nigh, Peter A McCullough, February 2023 link archive General
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has caused the pandemic of the coronavirus induced disease 2019 (COVID-19) with evolving variants of concern. It remains urgent to identify novel approaches against broad strains of SARS-CoV-2, which infect host cells via the entry receptor angiotensin-converting enzyme 2 (ACE2). Herein, we report an increase in circulating extracellular vesicles (EVs) that express ACE2 (evACE2) in plasma of COVID-19 patients, which levels are associated with severe pathogenesis. Importantly, evACE2 isolated from human plasma or cells neutralizes SARS-CoV-2 infection by competing with cellular ACE2. Compared to vesicle-free recombinant human ACE2 (rhACE2), evACE2 shows a 135-fold higher potency in blocking the binding of the viral spike protein RBD, and a 60- to 80-fold higher efficacy in preventing infections by both pseudotyped and authentic SARS-CoV-2. Consistently, evACE2 protects the hACE2 transgenic mice from SARS-CoV-2-induced lung injury and mortality. Furthermore, evACE2 inhibits the infection of SARS-CoV-2 variants (α, β, and δ) with equal or higher potency than for the wildtype strain, supporting a broad-spectrum antiviral mechanism of evACE2 for therapeutic development to block the infection of existing and future coronaviruses that use the ACE2 receptor.
nature.com [2023-03-13] Lamiaa El-Shennawy, Andrew D. Hoffmann, ..., Huiping Liu, 20 January 2022 link archive General
The recent COVID-19 pandemic is a treatment challenge in the acute infection stage but the recognition of chronic COVID-19 symptoms termed post-acute sequelae SARS-CoV-2 infection (PASC) may affect up to 30% of all infected individuals. The underlying mechanism and source of this distinct immunologic condition three months or more after initial infection remains elusive. Here, we investigated the presence of SARS-CoV-2 S1 protein in 46 individuals. We analyzed T-cell, B-cell, and monocytic subsets in both severe COVID-19 patients and in patients with post-acute sequelae of COVID-19 (PASC). The levels of both intermediate (CD14+, CD16+) and non-classical monocyte (CD14Lo, CD16+) were significantly elevated in PASC patients up to 15 months post-acute infection compared to healthy controls (P=0.002 and P=0.01, respectively). A statistically significant number of non-classical monocytes contained SARS-CoV-2 S1 protein in both severe (P=0.004) and PASC patients (P=0.02) out to 15 months post-infection. Non-classical monocytes were sorted from PASC patients using flow cytometric sorting and the SARS-CoV-2 S1 protein was confirmed by mass spectrometry. Cells from 4 out of 11 severe COVID-19 patients and 1 out of 26 also contained SARS-CoV-2 RNA. Non-classical monocytes are capable of causing inflammation throughout the body in response to fractalkine/CX3CL1 and RANTES/CCR5.
SARS-CoV-2, the causative agent of COVID-19 disease, has resulted in the death of millions worldwide since the beginning of the pandemic in December 2019. While much progress has been made to understand acute manifestations of SARS-CoV-2 infection, less is known about post-acute sequelae of COVID-19 (PASC). We investigated the levels of both Spike protein (Spike) and viral RNA circulating in patients hospitalized with acute COVID-19 and in patients with and without PASC. We found that Spike and viral RNA were more likely to be present in patients with PASC. Among these patients, 30% were positive for both Spike and viral RNA; whereas, none of the individuals without PASC were positive for both. The levels of Spike and/or viral RNA in the PASC+ve patients were found to be increased or remained the same as in the acute phase; whereas, in the PASC−ve group, these viral components decreased or were totally absent. Additionally, this is the first report to show that part of the circulating Spike is linked to extracellular vesicles without any presence of viral RNA in these vesicles. In conclusion, our findings suggest that Spike and/or viral RNA fragments persist in the recovered COVID-19 patients with PASC up to 1 year or longer after acute SARS-CoV-2 infection.
This study points to the pressing clinical need for the US FDA to grant in vitro diagnostics companies approvals to market blood assays for Spike protein and hopefully both viral and vaccine RNA and mRNA. In the meantime, there is now support to measure d-dimer in post COVID patients as weak surrogate of circulating Spike.
onlinelibrary.wiley.com [2023-03-13] Vaughn Craddock, Aatish Mahajan, Leslie Spikes, Balaji Krishnamachary, Anil K. Ram, Ashok Kumar, Ling Chen, Prabhakar Chalise, Navneet K. Dhillon, February 9, 2023 link archive General
The diagnosis of postacute sequelae of coronavirus disease 2019 (PASC) poses an ongoing medical challenge. To identify biomarkers associated with PASC we analyzed plasma samples collected from PASC and coronavirus disease 2019 patients to quantify viral antigens and inflammatory markers. We detect severe acute respiratory syndrome coronavirus 2 spike predominantly in PASC patients up to 12 months after diagnosis.
Strong Rationale for Empiric Base Spike Detox Regimen
Approximately 15% of patients took one or more injections of COVID-19 vaccine products and now have had COVID-19 illness and are suffering from persistent symptoms or new medical diseases. Of those ~94% received mRNA in Pfizer or Moderna products. Several studies have show that symptoms after COVID-19, most of whom also had baseline or subsequent vaccination, are directly related to persistent circulating Spike protein.
Swank et al, from Harvard University, found circulating Spike protein and or nucleocapsid in the blood of 65% of patients with long-COVID symptoms (post-acute sequelae symptoms) some of whom were unfortunately vaccinated even after being sick. These data imply the symptoms are driven by persistent fragments of the SARS-CoV-2 virus and Spike protein from repeated injections.
Base Spike Detox (BSD) is an empiric regimen designed to assist the body in breaking down the Spike protein and allowing natural clearance of protein fragments through the reticuloendothelial system. All three components have considerable support from the preclinical and clinical literature. Other agents can be added including N-acetylcysteine, but they should not be substituted for these three as the base of treatment (3-12+ months):
More information on Peter McCullough & treating the vaccine-injured
pubmed.ncbi.nlm.nih.gov [2023-08-14] Zoe Swank, Yasmeen Senussi, ..., David R Walt, February 2023 link archive General
In this two-part paper, we aim to give an overview on COVID-19 related abnormal blood clots, how they form, how to detect them early, and how they're being treated
Strange Clots
Since mid-2021, unusual, lengthy blood clots found in the vessels of COVID-19 patients and jab recipients have been reported across the world.
Fibrous Clots found in corpses by Richard Hirschman (Courtesy of Richard Hirschman)
“We as embalmers are seeing some strange clots since the COVID outbreak. These clots are very rubbery feeling and very long as they exit the veins that we use during the embalming procedure. They really appear to be like earthworms. I have never seen this in my career until now,” Larry Mills, a licensed embalmer and funeral director in the State of Alabama, told The Epoch Times.
Other embalmers confirmed similar findings and spoke on the condition of anonymity.
Richard Hirschman, Alabama funeral director and embalmer since 2001, was one of the first to bring attention to this phenomenon. He said that prior to COVID perhaps 5 to 10 percent of people had these clots. Now more than half of the bodies he sees have them.
One embalmer, licensed since 2001, said in an interview, “I can tell you with certainty that the clots Richard has shown online are a phenomenon that I have not witnessed until probably the middle of last year. That is pretty much all I have to say about it. I have no knowledge as to what is causing the clots, but they did seemingly start showing up around the middle of 2021.”
[...]
theepochtimes.com [2022-11-06] Dr. Yuhong Dong, Dr. Jordan Vaughn, Nov 5 2022 link archive General
The pathophysiology of COVID-19-associated coagulopathy is complex and not fully understood. SARS-CoV-2 spike protein (SP) may activate platelets and interact with fibrin(ogen). We aimed to investigate whether isolated SP can be present in clots retrieved in COVID-19 patients with acute ischemic stroke (by mechanical thrombectomy) and myocardial infarction. In this pilot study, we could detect SP, but not nucleocapsid protein, on platelets of COVID-19 patients’ thrombi. In addition, in all three COVID-19 thrombi analyzed for molecular biology, no SARS-CoV-2 RNA could be detected by real-time polymerase chain reaction. These data could support the hypothesis that free SP, besides the whole virus, may be the trigger of platelet activation and clot formation in COVID-19.
One of the remarkable observations about SARS-CoV-2 infection is the clinical manifestation of venous and arterial thrombosis. Multiple studies have described thrombotic complications of the infection including stroke, myocardial infarction, systemic arterial embolism, and deep venous thrombosis with pulmonary embolism. In my practice I have seen virtually every one of these complications. De Michele and colleagues studied patients with COVID-19 in 2020, before there were vaccines for the population.[i]
The key finding is that the SARS-CoV-2 spike protein latches on directly to the platelets in the blood clots taken from patients. This minus the full entire virus. So the spike protein functions on its own in the blood clotting sequelae. One could reasonably speculate that the other vaccine delivery platforms e.g. mRNA lipid-nano-particle, adeno-viral vector etc. does the same in terms of the spike protein (disassociated free spike).
jhoonline.biomedcentral.com [2022-12-06] Manuela De Michele, Giulia d’Amati, ..., Danilo Toni, 16 August 2022 link archive General
More information on COVID-19 vaccine adverse events & blood clots
Virus entry into animal cells is initiated by attachment to target macromolecules located on host cells. The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) trimeric spike glycoprotein targets host angiotensin converting enzyme 2 to gain cellular access. The SARS-CoV-2 glycoprotein contains a neurotoxin-like region that has sequence similarities to the rabies virus and the HIV glycoproteins, as well as to snake neurotoxins, which interact with nicotinic acetylcholine receptor (nAChR) subtypes via this region. Using a peptide of the neurotoxin-like region of SARS-CoV-2 (SARS-CoV-2 glycoprotein peptide [SCoV2P]), we identified that this area moderately inhibits α3β2, α3β4, and α4β2 subtypes, while potentiating and inhibiting α7 nAChRs. These nAChR subtypes are found in target tissues including the nose, lung, central nervous system, and immune cells. Importantly, SCoV2P potentiates and inhibits ACh-induced α7 nAChR responses by an allosteric mechanism, with nicotine enhancing these effects. Live-cell confocal microscopy was used to confirm that SCoV2P interacts with α7 nAChRs in transfected neuronal-like N2a and human embryonic kidney 293 cells. The SARS-CoV-2 ectodomain functionally potentiates and inhibits the α7 subtype with nanomolar potency. Our functional findings identify that the α7 nAChR is a target for the SARS-CoV-2 glycoprotein, providing a new aspect to our understanding of SARS-CoV-2 and host cell interactions, in addition to disease pathogenesis.
[...]
jbc.org [2023-05-31] Brittany C.V. O’Brien, Lahra Weber, Karsten Hueffer, Maegan M. Weltzin, MAY 2023 link archive General
SARS induced Death in mice via dysfunction of the Medulla via the OLFACTORY NERVE
Viral antigen distribution in the brain following intranasal inoculation. Brains were harvested from mice infected intranasally with 2.4 × 104 PFU and stained for viral antigen. (A to C) Antigen distribution in the brain at 60 h (A) and 3 (B), 4 (C), and 5 (D) days p.i. (E to J) The brain stem (E, G, and I) and hypothalamus (F, H, and J) were examined for viral antigen and inflammation. (E and F) Naïve controls. (G and H) SARS-CoV-infected brains exhibited antigen exclusively in neurons with no obvious inflammation at day 6 p.i. (compare to naïve controls). (I and J) JHMV-infected brains showed less extensive neuronal infection but severe perivascular inflammation (closed arrows) and meningitis (open arrows) at day 6 p.i. Original magnifications: ×1 (A to D) and ×5 (E to J).
Why this has not previously come to light and been discussed is beyond me. As you know, I have been researching the demyelination hypothesis as the cause of the Sudden Cardiac Deaths. I have discovered that the original SARS was able to induce Neuronal Death in the Medulla (cardiorespiratory center) resulting in the death of the subject.
[...]
wmcresearch.substack.com [2023-05-31] Walter M Chesnut, May 30, 2023 link archive General
The COVID-19 pandemic caused much illness, many deaths, and profound disruption to society. The production of 'safe and effective' vaccines was a key public health target. Sadly, unprecedented high rates of adverse events have overshadowed the benefits. This two-part narrative review presents evidence for the widespread harms of novel product COVID-19 mRNA and adenovectorDNA vaccines and is novel in attempting to provide a thorough overview of harms arising from the new technology in vaccines that relied on human cells producing a foreign antigen that has evidence of pathogenicity. This first paper explores peer-reviewed data counter to the 'safe and effective' narrative attached to these new technologies. Spike protein pathogenicity, termed 'spikeopathy', whether from the SARS-CoV-2 virus or produced by vaccine gene codes, akin to a 'synthetic virus', is increasingly understood in terms of molecular biology and pathophysiology. Pharmacokinetic transfection through body tissues distant from the injection site by lipid-nanoparticles or viral-vector carriers means that 'spikeopathy' can affect many organs. The inflammatory properties of the nanoparticles used to ferry mRNA; N1-methylpseudouridine employed to prolong synthetic mRNA function; the widespread biodistribution of the mRNA and DNA codes and translated spike proteins, and autoimmunity via human production of foreign proteins, contribute to harmful effects. This paper reviews autoimmune, cardiovascular, neurological, potential oncological effects, and autopsy evidence for spikeopathy. With many gene-based therapeutic technologies planned, a re-evaluation is necessary and timely.
Seven Australian Authors Publish Comprehensive Peer-Reviewed Paper Concluding Genetic Vaccines Must be Pulled
People commonly ask me for “comprehensive” publications on vaccine side effects. It is fair to point out that the SARS-CoV-2 Spike protein is contained in the virus and it is uncontrollably produced by the mRNA and adenoviral DNA COVID-19 vaccines. Because the vaccines failed to stop COVID-19, most vaccinated persons have had the illness, thereby having multiple Spike protein exposures.
Parry, et al, published a comprehensive review on the litany of Spike-protein diseases that occur after its widespread distribution in the body. Here are some of their evidence based teaching points:
SARS-CoV-2 spike protein is pathogenic, whether from the virus or created from genetic code in mRNA and adenovector DNA vaccines.
Biodistribution rodent study data show lipid nanoparticles carry mRNA to all organs and cross blood-brain and blood-placenta barriers. Some of these tissues are likely to be impervious to viral infection; therefore, the biohazard is particularly from vaccination.
Lipid-nanoparticles have inflammatory properties.
The modification of mRNA with N1-methylpseudouridine for increased stability leads to the production of spike proteins for months. It is uncertain how many cells and from which organs mRNA spike proteins are produced, and therefore, the exact effective dose delivered per vaccine vial is unknown.
The long-term fate of mRNA within cells is currently unknown.
The mRNA and adenovector DNA vaccines act as ‘synthetic viruses’.
In the young and healthy, and even in many older individuals with vulnerable comorbidities, the encoding-based COVID-19 vaccines will likely transfect a far more diverse set of tissues than infection by the virus itself.
Evidence suggests reverse transcription of mRNA into a DNA copy is possible. This further suggests the possibility of intergenerational transmission if germline cells incorporate the DNA copy into the host genome.
Production of foreign proteins such as spike protein on cell surfaces can induce autoimmune responses and tissue damage. This has profoundly negative implications for any future mRNA-based drug or vaccine.
The spike protein exerts its pathophysiological effects (‘spikeopathy’) via several mechanisms that lead to inflammation, thrombogenesis, and endotheliitis-related tissue damage and prion-related dysregulation. Interaction of the vaccine-encoded spike protein with ACE-2, P53 and BRCA1 suggests a wide range of possible biological interference with oncological potential.
Adverse event data from official pharmacovigilance databases, an FDA-Pfizer report obtained via FOI, show high rates and multiple organ systems affected: primarily neurological, cardiovascular, and reproductive.
Pfizer and Moderna mRNA COVID-19 vaccines’ clinical trial data independently interpreted has been peer-review and published to show an unfavourable risk/benefit, especially in the non-elderly. The risks for children clearly outweigh the benefits.
Repeated COVID-19 vaccine booster doses appear to induce tolerance and may contribute to recurrent COVID-19 infection and ‘long COVID’.
“The SARS-CoV-2 pandemic has revealed deficiencies in public health and medicines regulatory agencies. A root cause analysis is needed for what now appears a rushed response to an alarming infectious disease pandemic. Treatment modalities for ‘spikeopathy’-related pathology in many organ systems, require urgent research and provision to millions of sufferers of long-term COVID-19 vaccine injuries. We also advocate for the suspension of gene-based COVID-19 vaccines and lipid-nanoparticle carrier matrices, and other vaccines based on mRNA or viral-vector DNA technology. A safer course is to use vaccines with well-tested recombinant protein, attenuated or inactivated virus technologies, of which there are now many for vaccinating against SARS-CoV-2.”
pubmed.ncbi.nlm.nih.gov [2023-09-05] Peter I Parry, Astrid Lefringhausen, ..., Julian Gillespie, August 2023 link archive General
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has led to the coronavirus disease 2019 (COVID-19) pandemic, severely affecting public health and the global economy. Adaptive immunity plays a crucial role in fighting against SARS-CoV-2 infection and directly influences the clinical outcomes of patients. Clinical studies have indicated that patients with severe COVID-19 exhibit delayed and weak adaptive immune responses; however, the mechanism by which SARS-CoV-2 impedes adaptive immunity remains unclear. Here, by using an in vitro cell line, we report that the SARS-CoV-2 spike protein significantly inhibits DNA damage repair, which is required for effective V(D)J recombination in adaptive immunity. Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site. Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.
Related review/commentary: Welcome to Gilead, Dr Ah Kahn Syed, July 30, 2022
So when Jiang and Mei designed an experiment to look at the possibility that the SARS-CoV-2 proteins might impact this pathway in lymphocytes they were doing an experiment that was of vital importance to world’s population.
What did they find? Well, unfortunately something really important. That is, of all the proteins produced by the SARS-CoV-2 virus, one of them - the spike protein - obliterated the DNA repair mechanism in lymphocytes. Yeah, that’s really bad. Here is the graph from the paper showing the level of “HR efficiency” (i.e. homologous repair efficiency, i.e. the ability of the cell to repair DNA) seen with the different proteins of the virus. The spike protein was so toxic to this pathway that it knocked 90% of it out. This is an environment that is almost guaranteed to cause cancer.
pubmed.ncbi.nlm.nih.gov [2023-02-21] Hui Jiang, Ya-Fang Mei, October 2021 link archive General
The recently identified, globally predominant SARS-CoV-2 Omicron variant (BA.1) is highly transmissible, even in fully vaccinated individuals, and causes attenuated disease compared with other major viral variants recognized to date. The Omicron spike (S) protein, with an unusually large number of mutations, is considered the major driver of these phenotypes. We generated chimeric recombinant SARS-CoV-2 encoding the S gene of Omicron in the backbone of an ancestral SARS-CoV-2 isolate and compared this virus with the naturally circulating Omicron variant. The Omicron S-bearing virus robustly escapes vaccine-induced humoral immunity, mainly due to mutations in the receptor binding motif (RBM), yet unlike naturally occurring Omicron, efficiently replicates in cell lines and primary-like distal lung cells. In K18-hACE2 mice, while Omicron causes mild, non-fatal infection, the Omicron S-carrying virus inflicts severe disease with a mortality rate of 80%. This indicates that while the vaccine escape of Omicron is defined by mutations in S, major determinants of viral pathogenicity reside outside of S.
biorxiv.org [2022-10-17] Da-Yuan Chen, Devin Kenney, Chue-Vin Chin, ..., Nicholas A Crossland, Florian Douam, Mohsan Saeed, October 14, 2022 link archive General
Researchers added Omicron's spike protein to the original Wuhan Covid strain
Omicron's spike is highly mutated which made it the most infectious variant ever
Eight in 10 mice infected with the lab-created strain died at Boston University lab
Boston University scientists were today condemned for 'playing with fire' after it emerged they had created a lethal new Covid strain in a laboratory.
DailyMail.com revealed the team had made a hybrid virus — combining Omicron and the original Wuhan strain — that killed 80 per cent of mice in a study.
The revelation exposes how dangerous virus manipulation research continues to go on even in the US, despite fears similar practices may have started the pandemic.
Professor Shmuel Shapira, a leading scientist in the Israeli Government, said: 'This should be totally forbidden, it's playing with fire.'
Gain of function research - when viruses are purposefully manipulated to be more infectious or deadly - is thought to be at the center of Covid's origin.
A Chinese laboratory located just miles from the first cluster of cases carried out similar research on bat coronaviruses.
But the practice has been largely restricted in the US since 2017.
Dr Richard Ebright, a chemist at Rutgers University in New Brunswick, New Jersey, told DailyMail.com that: 'The research is a clear example of gain of function research.
He added: 'If we are to avoid a next lab-generated pandemic, it is imperative that oversight of enhanced potential pandemic pathogen research be strengthened.'
[...]
dailymail.co.uk [2022-10-19] CAITLIN TILLEY, MANSUR SHAHEEN, 17 October 2022 link archive General
According to a new paper just made public, researchers at Boston University were able to combine the spike protein from Omicron with the original strain of the virus, to create a new chimera strain that was so deadly it killed 80 percent of the humanized mice that they were testing on.
Using grant funding from both the NIH and the NIAID, the sub-agency led by Dr. Anthony Fauci, these scientists were able to cobble together a new strain of COVID. They dubbed their new creation Omicron S.
[...]
theepochtimes.com [2022-10-19] ROMAN BALMAKOV, October 18, 2022 link archive General
Boston University issued a statement Tuesday defending its research of a COVID-19 Omicron strain when they took the variant’s spike protein and attached it to the original COVID-19 strain, leading to a higher mortality rate in a certain species of mice, triggering concern among lawmakers.
“The Omicron S-bearing virus robustly escapes vaccine-induced humoral immunity, mainly due to mutations in the receptor-binding motif… while Omicron causes mild, non-fatal infection, the Omicron S-carrying virus inflicts severe disease with a mortality rate of 80 percent,” the preprint study said.
One lawmaker, Sen. Roger Marshall (R-Kan.), said that the research entailed “lethal gain of function virus research” that creates the “potential to kill more people than any singular nuclear weapon.” Marshal, a doctor, added that “viruses have managed to escape even the most secure labs” and said such “research must stop immediately while the risks and benefits can be investigated.”
Meanwhile, Emily Erbelding, director of the National Institute of Allergy and Infectious Diseases’s division of microbiology and infectious diseases, told Stat News that the Boston University’s grant application didn’t specify that researchers wanted to perform this work and the group did not say it was performing experiments to possible enhance a COVID-19 variant. An investigation is now underway, she said.
Boston University issued a lengthy statement defending its research and said critics have misrepresented the goals of the study while refuting allegations that the study involved gain-of-function research, which can make a pathogen more deadly or transmissible.
“The research was reviewed and approved by the Institutional Biosafety Committee (IBC), which consists of scientists as well as local community members,” the statement from Boston University said. “The Boston Public Health Commission also approved the research. Furthermore, this research mirrors and reinforces the findings of other, similar research performed by other organizations, including the FDA. Ultimately, this research will provide a public benefit by leading to better, targeted therapeutic interventions to help fight against future pandemics.”
Certain reports about the study were “false and inaccurate,” Boston University official Ronald Corley said in a statement. A report from the Daily Mail, he alleged, took the “80 percent” line out of context.
“We want to address the false and inaccurate reporting about Boston University COVID-19 research, which appeared today in the Daily Mail,” said the statement. “First, this research is not gain-of-function research, meaning it did not amplify the Washington state SARS-CoV-2 virus strain or make it more dangerous. In fact, this research made the virus replicate less dangerous.”
Lab Escape?
Addressing concerns that the manipulated COVID-19 Omicron strain could escape Boston University’s laboratory, Corley said the school takes safety seriously.
“We take our safety and security of how we handle pathogens seriously, and the virus does not leave the laboratory in which it’s being studied,” he said. “Our whole goal is for the public’s health. And this study was part of that, finding what part of the virus is responsible for causing severe disease. If we can understand that, we can then develop the tools that we need to develop better therapeutics.”
However, one doctor interviewed by the Daily Mail expressed alarm over the research.
“The issue is what you’re going to be using [the labs] for. If they’re for diagnostic purposes, then you need them. But I don’t think every country needs a BSL-4,” Dr. Paul Hunter, an expert in infectious diseases at England’s University of East Anglia, said, referring to the top level of biosecurity used in laboratories.
“If they start having a dual purpose for research that has offensive military implications, that is the concern,” he said.
[...]
theepochtimes.com [2022-10-19] Jack Phillips, October 18, 2022 link archive General
More information on Boston University's chimeric Omicron spike research
The COVID-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has resulted in over 6 million deaths worldwide. The high variability in COVID-19 symptoms remains one of the most interesting mysteries of the pandemic. Genetic and environmental factors are likely to be key determinants of COVID-19 symptomatology. Here, we explored ACE2 as a genetic determinant for SARS-CoV-2 infection and COVID-19 symptomatology. Each human genome encodes two alleles of ACE2, which encodes the cell entry receptor for SARS-CoV-2. Here, we determined whether naturally occurring human ACE2 (hACE2) polymorphisms in the human population affect SARS-CoV-2 infection and the severity of COVID-19 symptoms. ACE2 variants S19P, I21V, E23K, K26R, K31R, N33I, H34R, E35K, and T92I showed increased virus infection compared to wild-type ACE2; thus, these variants could increase the risk for COVID-19. In contrast, variants D38V, Y83H, I468V, and N638S showed reduced infection, indicating a potential protective effect. hACE2 variants K26R and T92I increased infection by three-fold without changing the levels of ACE2 on the surface of the cells, suggesting that these variants may increase the risk of severe COVID-19. On the contrary, hACE2 variants D38V and Y83H decreased SARS-CoV-2 infection by four- and ten-fold, respectively, without changing surface expression, suggesting that these variants may protect against severe COVID-19. Remarkably, all protective hACE2 Polymorphisms were found almost exclusively in Asian populations, which may provide a partial explanation for the low COVID-19 mortality rates in Asian countries. Thus, hACE2 polymorphisms may modulate susceptibility to SARS-CoV-2 in the host and partially account for the differences in severity of COVID-19 among different ethnic groups.
Just in case anyone like CNN was wondering: Host susceptibility to COVID-19 varies with genetics and ethnicity usually correlates with genetics. The host susceptibility variation is based on differences in ACE2 receptors.
pubmed.ncbi.nlm.nih.gov [2023-07-17] Pan Hu, Vanessa L Bauer, Sara L Sawyer, Felipe Diaz-Griffero, June 2022 link archive General
Background: Coronavirus Disease 2019 (COVID-19), caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has now been confirmed worldwide. Yet, COVID-19 is strangely and tragically selective. Morbidity and mortality due to COVID19 rise dramatically with age and co-existing health conditions, including cancer and cardiovascular diseases. Human genetic factors may contribute to the extremely high transmissibility of SARS-CoV-2 and to the relentlessly progressive disease observed in a small but significant proportion of infected individuals, but these factors are largely unknown.
Main body: In this study, we investigated genetic susceptibility to COVID-19 by examining DNA polymorphisms in ACE2 and TMPRSS2 (two key host factors of SARS-CoV-2) from ~ 81,000 human genomes. We found unique genetic susceptibility across different populations in ACE2 and TMPRSS2. Specifically, ACE2 polymorphisms were found to be associated with cardiovascular and pulmonary conditions by altering the angiotensinogen-ACE2 interactions, such as p.Arg514Gly in the African/African-American population. Unique but prevalent polymorphisms (including p.Val160Met (rs12329760), an expression quantitative trait locus (eQTL)) in TMPRSS2, offer potential explanations for differential genetic susceptibility to COVID-19 as well as for risk factors, including those with cancer and the high-risk group of male patients. We further discussed that polymorphisms in ACE2 or TMPRSS2 could guide effective treatments (i.e., hydroxychloroquine and camostat) for COVID-19.
Conclusion: This study suggested that ACE2 or TMPRSS2 DNA polymorphisms were likely associated with genetic susceptibility of COVID-19, which calls for a human genetics initiative for fighting the COVID-19 pandemic.
[...]
ACE2 polymorphism analysis across different populations
[...] We found that the distribution of deleterious variants in ACE2 differs among 9 populations in gnomAD (v3). Specifically, 39% (24/61) and 54% (33/61) of deleterious variants in ACE2 occur in African/African-American (AFR) and Non-Finnish European (EUR) populations, respectively (Fig. 1b). Prevalence of deleterious variants among Latino/Admixed American (AMR), East Asian (EAS), Finnish (FIN), and South Asian (SAS) populations is 2–10%, while Amish (AMI) and Ashkenazi Jewish (ASJ) populations do not appear to carry such variants in ACE2 coding regions (Fig. 1b). Specifically, several variants, including p.Met383Thr, p.Pro389His, and p.Asp427Tyr, have been reported to slightly inhibit the interaction between ACE2 and the spike protein of SARS-CoV-1 [10], which caused the first global SARS-CoV-1 outbreak. [...]
We are currently witnessing a major epidemic caused by the 2019 novel coronavirus (2019- nCoV). The evolution of 2019-nCoV remains elusive. We found 4 insertions in the spike glycoprotein (S) which are unique to the 2019-nCoV and are not present in other coronaviruses. Importantly, amino acid residues in all the 4 inserts have identity or similarity to those in the HIV-1 gp120 or HIV-1 Gag. Interestingly, despite the inserts being discontinuous on the primary amino acid sequence, 3D-modelling of the 2019-nCoV suggests that they converge to constitute the receptor binding site. The finding of 4 unique inserts in the 2019-nCoV, all of which have identity /similarity to amino acid residues in key structural proteins of HIV-1 is unlikely to be fortuitous in nature. This work provides yet unknown insights on 2019-nCoV and sheds light on the evolution and pathogenicity of this virus with important implications for diagnosis of this virus.
LONDON, Feb 1 (Reuters) - Leading South African scientists are set to investigate COVID-19 and HIV in tandem, amid mounting evidence that the collision of the two pandemics could be generating new coronavirus variants.
reuters.com [2022-02-11] By Jennifer Rigby, February 1, 2022 link archive General
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the agent of a major global outbreak of respiratory tract disease known as coronavirus disease-2019 (COVID-19). SARS-CoV-2 infects mainly lungs and may cause several immune-related complications, such as lymphocytopenia and cytokine storm, which are associated with the severity of the disease and predict mortality1,2. The mechanism by which SARS-CoV-2 infection may result in immune system dysfunction is still not fully understood. Here we show that SARS-CoV-2 infects human CD4+ T helper cells, but not CD8+ T cells, and is present in blood and bronchoalveolar lavage T helper cells of severe COVID-19 patients. We demonstrated that SARS-CoV-2 spike glycoprotein (S) directly binds to the CD4 molecule, which in turn mediates the entry of SARS-CoV-2 in T helper cells. This leads to impaired CD4 T cell function and may cause cell death. SARS-CoV-2-infected T helper cells express higher levels of IL-10, which is associated with viral persistence and disease severity. Thus, CD4-mediated SARS-CoV-2 infection of T helper cells may contribute to a poor immune response in COVID-19 patients.
Coronavirus disease 2019 (COVID-19) has rapidly spread across the globe3,4, being declared a pandemic by the World Health Organization (WHO) on March 11th, 2020. COVID-19 has caused millions of deaths around the world. Most of the deaths are associated with acute pneumonia, cardiovascular complications, and organ failure due to hypoxia, exacerbated inflammatory responses and widespread cell death1,5. Individuals that progress to the severe stages of COVID-19 manifest marked alterations in the immune response, characterized by reduced overall protein synthesis, cytokine storm, lymphocytopenia and T cell exhaustion6–8. In addition to these acute effects on the immune system, a considerable proportion of infected individuals present low titers of neutralizing antibodies9,10. Moreover, the levels of antibodies against SARS-CoV-2 decay rapidly after recovery in part of the infected individuals11, suggesting that SARS-CoV-2 infection may exert profound and long-lasting complications to adaptive immunity. Recently, it has been shown that SARS-CoV-2 is able to infect lymphocytes12,13. In this context, it is urgent to characterize the replicative capacity and the effects of SARS-CoV-2 replication in different immune cells, especially those involved with the formation of immunological memory and effective adaptive response, such as CD4+ T lymphocytes.
In what has been proposed to be the canonical mechanism of SARS-CoV-2 infection, the spike glycoprotein of SARS-CoV-2 (sCoV-2) binds to the host angiotensin-converting enzyme 2 (ACE2), after which it is cleaved by TMPRSS214. While TMPRSS2 is ubiquitously expressed in human tissues (Extended Data Fig. 1), ACE2 is mainly expressed in epithelial and endothelial cells, as well as in the kidney, testis and small intestine (Extended Data Fig.1). Still, a wide variety of cell types are potentially infected by SARS-CoV-215–18, even though some of these cells express very low levels of ACE2. We showed this is the case for lymphocytes (Extended Data Fig. 2). These findings suggest that either SARS-CoV-2 uses alternative mechanisms to enter these cells or that auxiliary molecules at the plasma membrane may promote infection by stabilizing the virus until it interacts with ACE2. In agreement with the latter, binding of sCoV-2 to certain cell surface proteins facilitates viral entry19,20.
[...]
Since the structures of the spike of SARS-CoV-1 (sCoV-1) and the sCoV-2 proteins are similar21,22, we used the P-HIPSTer algorithm to uncover human proteins that putatively interact with spike23. Seventy-one human proteins were predicted to interact with sCoV-1 (Extended Data Fig. 3). We then cross-referenced the proteins with five databases of plasma membrane proteins to identify the ones located on the cell surface (see Methods for details). CD4 was the only protein predicted to interact with sCoV-1 that appeared in all five databases (Extended Data Fig.3). CD4 is expressed mainly in T helper lymphocytes and has been shown to be the co-receptor to HIV24. Since CD4+ T lymphocytes orchestrate innate and adaptive immune response25,26, infection of CD4+ T cells by SARS-CoV-2 could explain lymphocytopenia and dysregulated inflammatory response in severe COVID-19 patients. Moreover, from an evolutionary perspective, infection of CD4+ T cells represents an effective mechanism for viruses to escape the immune response27.
[...]
medrxiv.org [2023-08-09] Natália S. Brunetti, Gustavo G. Davanzo, ..., Alessandro S. Farias, January 11, 2023 link archive General
? The puzzle pieces continue to fall into place, and a significant new puzzle piece dropped last week, in the form of a preprint published to MedRxIV on July 31st, titled “SARS-CoV-2 Uses CD4 to Infect T Helper Lymphocytes.”
Although “just” a preprint, it features no fewer than seventy-seven authors. And it has already gathered three positive peer reviews. Let’s start with their conclusion, and then try to unpack what it means. The study’s admittedly obscure conclusion:
We demonstrated that SARS-CoV-2 spike glycoprotein (S) directly binds to the CD4 molecule, which in turn mediates the entry of SARS-CoV-2 in T helper cells. This leads to impaired CD4 T cell function and may cause cell death. SARS-CoV-2-infected T helper cells express higher levels of IL-10, which is associated with viral persistence and disease severity. Thus, CD4-mediated SARS-CoV-2 infection of T helper cells may contribute to a poor immune response in COVID-19 patients.
The researchers figured this out by first using sophisticated genetic software to analyze covid’s RNA. The results showed that covid’s spike protein potentially interacts with 77 different human tissues. But, after they filtered the results for proteins found on the outside of human cells, which are accessible to the spike, they found only one match: something called CD4 helper cells.
Then the researchers proved that covid does target CD4 cells in vivo, including by infecting previously un-infected blood, and by testing blood samples from recovering covid patients. They were very careful and the result seems pretty well established. So it almost seems like the spike was designed to attack this one particular type of cell. But what is it?
CD4 cells are also called “T helper cells.” They are a type of white blood cell playing a critical role in the immune system. Specifically, CD4 is a key part of the adaptive immune response, which is the body's initial defense mechanism against infections.
In fact, at bottom your immune system is coordinated by CD4 cells, which are the front line of recognizing invasive pathogens like viruses and bacteria. The CD4 cells raise an alarm, prompting other types of immune cells to respond appropriately. CD4 accomplishes this by releasing ‘signaling molecules’ called cytokines. In turn, cytokines regulate the activity of more complex immune cells.
Not to beat a dead horse, but CD4 cells are especially important in coordinating the immune response against infections, and they are central to the body's ability to remember and respond to specific pathogens. However, certain viruses, like HIV, specifically target and infect CD4 cells themselves, thereby knocking out the frontline immune response and weakening the overall immune system — which alarmingly creates increased vulnerability to other opportunistic infections.
Opportunistic infections like monkeypox, Hansen’s disease, RSV, and so on. Just to name a few, at random.
So what does all this mean, beyond a weakened immune system? The researchers speculated:
Infection of CD4+ T cells by SARS-CoV-2 could explain lymphocytopenia and dysregulated inflammatory response in severe COVID-19 patients. Moreover, from an evolutionary perspective, infection of CD4+ T cells represents an effective mechanism for viruses to escape the immune response.
In other words, the spike protein’s CD4-attacking feature seems almost designed to avoid the human immune response. Just what you’d want in a bioweapon, for example.
Once inside the CD4 cell, the covid virus weakens and kills it, destroying part of the immune system each time it happens. Worse, this process increases systemic levels of an inflammatory cytokine called Interleukin-10 (IL-10 ), which is associated with “viral persistence,” meaning an IL-10 inflammation makes it harder for the body to clear an infection. So covid — specifically its spike protein — hits the immune system two different ways.
Ultimately, the authors conceded that we don’t know how long the effect lasts:
How long these alterations in T cell function persist in vivo and whether they have long-lasting impacts on adaptive immunity remains to be determined.
But we do know one thing. Every time someone takes a jab, they reset their doses of spike, flooding their bodies with another few months worth. Back at the time the FDA “approved” the safest and most effective vaccines in human history, this effect of attacking the immune system through CD4 was unknown. One wonders, doesn’t one, whether it would have made any difference had these dangerous knock-on effects been publicly known.
Anyway, and most significantly, the authors ended by proposing further research to help develop clinical treatments based on knowing about covid’s CD4-targeted behavior:
Hence, avoiding T cell infection by blocking SARS-CoV-2—CD4 interaction and boosting T cell resistance against SARS-CoV-2 might represent complementary therapeutic approaches to preserve immune response integrity and prevent patients from progressing to the severe stages of COVID-19.
In other words — millions of lives might have been saved had we had known about this problem early in the pandemic. But instead, all those people were given useless remdesivir treatments and smothered by ventilators. And they died in large numbers.
Now let’s take a look at the indisputable evidence that damns the United States government, especially its bloated health agencies.
? Guess what the evidence shows? Fauci and the NIH knew all along. On January 30th of 2020 — right at the start of the pandemic — a group of Indian researchers published a study, which was nearly immediately forced to be withdrawn, that claimed HIV genes were found inserted into covid’s RNA. HIV also targets the CD4 cell.
So the problem wasn’t hard to find. But even if the CDC and the NIH somehow never saw the withdrawn study, a FOIA’d email dated Tuesday, February 4th, 2020, proves that reprehensible human cockroach Anthony Fauci was separately and directly told about this immuno-destructive feature of covid, at the time when the knowledge could have saved countless lives, but he arrogantly dismissed it. (Or worse, he and the NIH actively suppressed the information.)
Here’s the proof:
There was no good reason for the NIH to fail to follow up on this email. Even bypassing Fauci’s dismissive tone, a tone — “this person” — suggesting the emailer should be submerged in the nearest septic tank until he stopped kicking, even overlooking all that: Fauci forwarded the email to NIH staff for action.
But nothing happened. It just went away.
Remember: as the new study suggested, we might have developed treatments to deal with CD4 infection and IL-10 cytokine expression, treatments that would have saved countless lives. Instead, what did the NIH do? Nothing. Or worse, they aggressively suppressed the discovery.
Maybe they suppressed it because of Fauci’s long, sordid history with HIV. Fauci needed another HIV scandal like a hole in the cranium.
Think about it. Even setting aside the panoply of conspiracy facts suggesting much darker motives, in early February of 2020 Fauci was looking at a brand-new (“novel”) coronavirus to play with. He probably knew full well that thousands of germaphobes would soon be 3D-printing idolic Fauci bobbleheads and setting up little Fauci shrines. The last thing Fauci wanted would’ve been to drag all that old HIV baggage into the covid pandemic.
If that happened, everybody would just be remembering how the bureaucratic human barnacle bungled the HIV pandemic.
And who knows? They might have even pulled him off the project, because of the awful optics. Worse, maybe that ridiculous buffoon Luc Montagnier might’ve been put in charge of the response. Montagnier’s Nobel prize for HIV should’ve been Fauci’s, if it weren’t for all those meddling gay Americans who muddled the waters so much.
But that’s not all. Not even close.
? Let’s not forget about the money. This clip compilation by pandemic heroine Texas Lindsay (may God bless her and keep her long upon the Earth) is relevant and mind-blowing. You might want to watch it twice. Lindsay’s five-minute clip assembled the entire story, but please don’t miss Fauci’s appearance expressing his 2019 desire, his “hope,” to “rapidly respond to something brand new.”
Here’s the point. Forget about ivermectin and hydroxychloroquine for a minute. If an effective treatment targeting covid’s deadliest unique mechanism of harm had been developed, a treatment that could have interrupted the destructive autoimmune cytokine storm by, say, blocking covid’s attack on CD4 cells, the entire pandemic would have been avoided.
And if that had happened, if the pandemic had been avoided, mass mail-in ballots wouldn’t have been authorized, Trump would have been re-elected, the NIH would never have earned billions, and millions of costly social security recipients would still be alive. Not to mention the losses to all the downstream pandemic beneficiaries like Amazon, Bill Gates, corporate media, social media, hospitals, military bio-contractors, and local governments that would never had gotten paid.
To a large group of amoral, devil-worshipping, government-enriched élites, that would have been a catastrophe.
? But it may even be worse than that. If, as the study suggests, covid includes HIV, and works like HIV, then it is possible that the worst is yet to come. HIV starts with cold-like symptoms, just like covid, but then remains dormant for 8-10 years before the truly serious immune deterioration begins.
The connections between covid and HIV aren’t new. Over the last two years, there have been any number of signs of similarities cropping up between HIV and covid, as well as increasing government interest in HIV. For just one example, you’ll recall last year’s push for everyone to get tested for HIV:
Or this headline from the Hill in January 2022:
[...]
? Now remember: we’ve proven Fauci and the NIH knew about covid’s HIV-like effects in February 2020. Yet they rabidly censored all discussion about the problem, even to the extent of shutting down all research or even speculation into the bioweapons design of the virus. After all, if covid was zoonotic (naturally evolved in bats) nobody would even consider something like this. In other words, don’t be silly, what do bats have to do with HIV?
Here’s the bottom line. The decision to include spike protein in the experimental shots may wind up being the most deadly, recklessly negligent, reprehensible, and ultimately horrifying decision ever to emerge from fevered imaginations of mediocre government scientists. Spike’s mechanism of attacking CD4 cells — directly attacking the immune system itself — should have been an absolute disqualifier for inclusion of spike protein in the jabs.
[...]
coffeeandcovid.com [2023-08-09] Jeff Childers, August 8, 2023 link archive General
Novel coronavirus disease 2019 (COVID-19) is the biggest threat to human being globally. The first case was identified in a patient with flu symptoms along with severe acute respiratory syndrome in Wuhan, China in December 2019 and now it has spread in more than 200 countries. COVID-19 is more lethal in the elderly and people with an underlying condition such as asthma, cancer, diabetes. Here we performed bioinformatic analysis to investigate the interaction of S2 subunit protein of SARS-nCoV-2 of novel coronavirus with tumor suppressor proteins p53 and BRCA-1/2. In this short communication we report the interaction between S2 subunit proteins with tumor suppressor proteins for the first time. This preliminary result will open up a new direction to investigate the effect of a novel coronavirus in cancer patients.
pubmed.ncbi.nlm.nih.gov [2023-09-21] Nishant Singh, Anuradha Bharara Singh, October 2020 link archive General
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and COVID-19 infection has led to worsened outcomes for patients with cancer. SARS-CoV-2 spike protein mediates host cell infection and cell-cell fusion that causes stabilization of tumor suppressor p53 protein. In-silico analysis previously suggested that SARS-CoV-2 spike interacts with p53 directly but this putative interaction has not been demonstrated in cells. We examined the interaction between SARS-CoV-2 spike, p53 and MDM2 (E3 ligase, which mediates p53 degradation) in cancer cells using an immunoprecipitation assay. We observed that SARS-CoV-2 spike protein interrupts p53-MDM2 protein interaction but did not detect SARS-CoV-2 spike bound with p53 protein in the cancer cells. We further observed that SARS-CoV-2 spike suppresses p53 transcriptional activity in cancer cells including after nutlin exposure of wild-type p53-, spike S2-expressing tumor cells and inhibits chemotherapy-induced p53 gene activation of p21(WAF1), TRAIL Death Receptor DR5 and MDM2. The suppressive effect of SARS-CoV-2 spike on p53-dependent gene activation provides a potential molecular mechanism by which SARS-CoV-2 infection may impact tumorigenesis, tumor progression and chemotherapy sensitivity. In fact, cisplatin-treated tumor cells expressing spike S2 were found to have increased cell viability as compared to control cells. Further observations on gamma-H2AX expression in spike S2-expressing cells treated with cisplatin may indicate altered DNA damage sensing in the DNA damage response pathway. The preliminary observations reported here warrant further studies to unravel the impact of SARS-CoV-2 and its various encoded proteins including spike on pathways of tumorigenesis and response to cancer therapeutics.
The authors report that the S2 component of the spike protein interferes with p53 signaling in cancer cells. There’s a protein called MDM2 that acts in tandem with p53: MDM2 ubiquitinates (protein synthesis/degradation stuff) p53, and p53 activates transcription of MDM2. I scratch your back, you scratch mine. See spike S2 component below in Figure 1.2
Figure 1: Spike-protein-mediated membrane fusion. Esteban Dodero-Rojas Jose N Onuchic Paul Charles Whitford (2021). Sterically confined rearrangements of SARS-CoV-2 Spike protein control cell invasion eLife 10:e70362. https://doi.org/10.7554/eLife.70362 The authors write:
The bottom line here is that the component of the spike protein of SARS-2, S2, responsible for cell entry as part of receptor-mediated endocytosis, messes up p53 activity. We all know by now that p53 - the guardian of the genome - assures that double-stranded DNA breaks are repaired and genome mutations limited, by surveillance of DNA and control of the cell cycle.
The suppressive effect of SARS-CoV-2 spike on p53-dependent gene activation provides a potential molecular mechanism by which SARS-CoV-2 infection may impact tumorigenesis, tumor progression and chemotherapy sensitivity.
This is the same spike S2 that is indeed encoded in the template that was used in the COVID modified mRNA shots.
Figure 2: Spike protein production by human cells via LNP/modified mRNA transfection. https://www.genome.gov/about-genomics/fact-sheets/Understanding-COVID-19-mRNA-Vaccines - Courtesy: National Human Genome Research Institute
The authors aren’t sure yet how S2 is doing this, ie: is it interrupting “p53 binding to the DNA promoters of the targets”, is it “inhibiting p53 transcriptional activity through post-translational modifications in p53”, or is it “altering other proteins that complex with p53”. They rightly point out that we need to do more work to find out.
Once again, this is the kind of thing that should have been done prior to using the spike protein as the coding template for the COVID-19 shots that we all so desperately needed.
biorxiv.org [2024-04-16] Shengliang Zhang, Wafik S. El-Deiry, April 15, 2024 link archive General
The present review aims to help the scientific community to better understand, in vitro and in vivo, COVID-19 compared to Monge disease (MD). The SARS-COV-2 or Corona-nanoparticles (NPs: 60-140nm) model based on nanosciences give an innovative understanding of virus nanotoxicity associated with violent inflammatory reactions and acute respiratory distress. Our analysis of COVID-19 suggests for the first time as far as we know that SARS-COV-2 use nanosciences laws such as virus agglomeration and mitochondria respiration toxicity induced by cluster virus-Heme. Moreover, the implication of age, gender, and ethnicity to COVID-19 must be confirmed by future studies compared to MD. The virus could use nano mechanisms to induce hypoxia via the generation of Heme-virus clusters mitigating micro coagulation implicated in acute respiratory distress and heart failure. Our analysis points to the presence of a possible link between hypoxia and COVID-19 pro-pulmonary complications.
cienciaworld.com [2022-03-24] (pdf doc) Amel Hanini, Ouajdi Souilem, Hafedh Abdelmelek, 27 July 2020 link archive General
- Link to Bioweapons -
Coronavirus Research
US Governement (NIAID) sponsored studies specifically focused on Bat, "SARS-like" Coronavirus originations and designations. (link)
Ralph Baric, an infectious-disease researcher at the University of North Carolina at Chapel Hill, last week (November 9) published a study on his team’s efforts to engineer a virus with the surface protein of the SHC014 coronavirus, found in horseshoe bats in China, and the backbone of one that causes human-like severe acute respiratory syndrome (SARS) in mice. The hybrid virus could infect human airway cells and caused disease in mice, according to the team’s results, which were published in Nature Medicine. [ archived link ]
The results demonstrate the ability of the SHC014 surface protein to bind and infect human cells, validating concerns that this virus—or other coronaviruses found in bat species—may be capable of making the leap to people without first evolving in an intermediate host, Nature reported. They also reignite a debate about whether that information justifies the risk of such work, known as gain-of-function research. “If the [new] virus escaped, nobody could predict the trajectory,” Simon Wain-Hobson, a virologist at the Pasteur Institute in Paris, told Nature.
In October 2013, the US government put a stop to all federal funding for gain-of-function studies, with particular concern rising about influenza, SARS, and Middle East respiratory syndrome (MERS). “NIH [National Institutes of Health] has funded such studies because they help define the fundamental nature of human-pathogen interactions, enable the assessment of the pandemic potential of emerging infectious agents, and inform public health and preparedness efforts,” NIH Director Francis Collins said in a statement at the time. “These studies, however, also entail biosafety and biosecurity risks, which need to be understood better.”
the-scientist.com [2020-06-17] Jef Akst, Nov 16, 2015 link archive Bioweapons
Exclusive information. Multiple highly regarded scientists who have studied C0R0NAVlRUS say that the VlRUS has been manipulated in labs to better attach to human cells. Turns out, research on that very thing was conducted here in the United States until the research was banned in 2013. In 2014, the research appears to have resumed through funding to several labs in China through payments to Eco Health Alliance. We break down the timeline.
Zhao was soon joined by bioweapons experts like Francis Boyle, prominent virologists Luc Montagnier and Judy Mikovits, followed by a growing array of scholars, scientists and academics from around the world who all assessed that the virus’ apparent gene sequencing implied human handiwork. While all agreed that COVID appeared to have originated from a lab, it was still unclear whether that lab was Chinese or controlled by the USA.
Another obvious question arose with this lab theory: Was it an accidental leak or was it consciously deployed?
Since pandemic war game operations had become a normalized part of western geopolitical life from the early days of Dark Winter in 2000 to the Rockefeller Foundation’s 2011 Lock Step to the World Economic Forum’s Event 201 (and dozens more in between), the likelihood of conscious deployment was a very serious possibility.
1) TMPRSS2 gene expressions which have a role in the susceptibility to SARS-CoV-2 are "Less frequent in Eastern Asians but more frequent in Europeans" https://ncbi.nlm.nih.gov/pmc/articles/PMC7417663/
2) "Large variations in binding energy in different ACE2 variants towards SARS-CoV-2S protein have been reported, ranking from high to low: G211R (European, South Asian), D206G (European), K341R (African, African American), R219C (South Asian), I468V (East Asian), K26R (Ashkenazi Jews)" https://sciencedirect.com/science/article/pii/S006524232100055X
Israel is reportedly developing a biological weapon that would harm Arabs while leaving Jews unaffected, according to a report in London's Sunday Times. The report, citing Israeli military and western intelligence sources, says that scientists are trying to identify distinctive genes carried by Arabs to create a genetically modified bacterium or virus. The "ethno-bomb" is […]
See related data elements:
New insights into genetic susceptibility of COVID-19: an ACE2 and TMPRSS2 polymorphism analysis
RFK Jr. says COVID may have been ‘ethnically targeted’ to spare Jews
Human ACE2 Polymorphisms from Different Human Populations Modulate SARS-CoV-2 Infection
The Truth Within RFK Jr's Statements About "Ethnically Targeted" Weapons
twitter.com [2023-07-16] Censored Men@CensoredMen, Jul 15, 2023 link archive General
If you count biosafety level 3 (BSL-3) labs, there are more than 200! And, that’s from a USA Today investigation back in 2015! Even more high-containment labs are operating now.
If you’re in Maryland near Washington, DC, like I am, you’re in the belly of the biolab beast where three BSL-4 and thirteen BSL-3 labs are in operation! We’ve already got a protest going every Wednesday at noon against Anthony Fauci, who runs several BSL-4 labs, including the NIAID Integrated Research Facility at Fort Detrick where the anthrax used in the 2001 false flag attacks is said to have originated. Three of the people involved in Amerithrax are key players in COVID-19. Former Fort Detrick commander David Franz who had a DARPA contract to create the attack anthrax now works for EcoHealth Alliance, the US partner and funder of the Wuhan Institute of Virology. Trump’s Assistant Secretary for Preparedness and Response Robert Kadlec helped Emergent Biosolutions profit off the 2001 attacks and COVID-19. Kadlec’s deputy, David Christian “Chris” Hassell was the FBI lab director who pinned the anthrax attacks on patsy Bruce Ivins. Hassell now serves as the only known member of the secret committee funding gain-of-function research.
Within 4 weeks following infection, 90-99% of individuals infected with the SARS-CoV-2 virus develop detectable neutralizing antibodies.
The strength and duration of the immune responses to SARS-CoV-2 are not completely understood and currently available data suggests that it varies by age and the severity of symptoms. Available scientific data suggests that in most people immune responses remain robust and protective against reinfection for at least 6-8 months after infection (the longest follow up with strong scientific evidence is currently approximately 8 months).
Some variant SARS-CoV-2 viruses with key changes in the spike protein have a reduced susceptibility to neutralization by antibodies in the blood. While neutralizing antibodies mainly target the spike protein, cellular immunity elicited by natural infection also target other viral proteins, which tend to be more conserved across variants than the spike protein. The ability of emerging virus variants (variants of interest and variants of concern) to evade immune responses is under investigation by researchers around the world.
There are many available serologic assays that measure the antibody response to SARS-CoV-2 infection, but at the present time, the correlates of protection are not well understood
apps.who.int [2021-06-17] (pdf doc) 10 May 2021 link archive General
People who recover from mild COVID-19 have bone-marrow cells that can churn out antibodies for decades, although viral variants could dampen some of the protection they offer.
nature.com [2021-06-28] Ewen Callaway, 26 May 2021 link archive General
Preexisting cross-reactivity to SARS-CoV-2 occurs in the absence of prior viral exposure. However, this has been difficult to quantify at the population level due to a lack of reliably defined seroreactivity thresholds. Using an orthogonal antibody testing approach, we estimated that about 0.6% of nontriaged adults from the greater Vancouver, Canada, area between May 17 and June 19, 2020, showed clear evidence of a prior SARS-CoV-2 infection, after adjusting for false-positive and false-negative test results. Using a highly sensitive multiplex assay and positive/negative thresholds established in infants in whom maternal antibodies have waned, we determined that more than 90% of uninfected adults showed antibody reactivity against the spike protein, receptor-binding domain (RBD), N-terminal domain (NTD), or the nucleocapsid (N) protein from SARS-CoV-2. This seroreactivity was evenly distributed across age and sex, correlated with circulating coronaviruses’ reactivity, and was partially outcompeted by soluble circulating coronaviruses’ spike. Using a custom SARS-CoV-2 peptide mapping array, we found that this antibody reactivity broadly mapped to spike and to conserved nonstructural viral proteins. We conclude that most adults display preexisting antibody cross-reactivity against SARS-CoV-2, which further supports investigation of how this may impact the clinical severity of COVID-19 or SARS-CoV-2 vaccine responses.
insight.jci.org [2021-06-28] Abdelilah Majdoubi, Christina Michalski, Sarah E. O’Connell, Sarah Dada, Sandeep Narpala, Jean Gelinas, Disha Mehta, Claire Cheung, Dirk F.H. Winkler, Manjula Basappa, Aaron C. Liu, ..., March 15, 2021 link archive General
Generating immunity against the SARS-CoV-2 coronavirus is of the utmost importance for bringing the COVID-19 pandemic under control, protecting vulnerable individuals from severe disease and limiting viral spread. Our immune systems protect against SARS-CoV-2 either through a sophisticated reaction to infection or in response to vaccination. A key question is, how long does this immunity last? Writing in Nature, Turner et al.1 and Wang et al.2 characterize human immune responses to SARS-CoV-2 infection over the course of a year.
There is ongoing discussion about which aspects of the immune response to SARS-CoV-2 provide hallmarks of immunity (in other words, correlates of immunological protection). However, there is probably a consensus that the two main pillars of an antiviral response are immune cells called cytotoxic T cells, which can selectively eliminate infected cells, and neutralizing antibodies, a type of antibody that prevents a virus from infecting cells, and that is secreted by immune cells called plasma cells. A third pillar of an effective immune response would be the generation of T helper cells, which are specific for the virus and coordinate the immune reaction. Crucially, these latter cells are required for generating immunological memory — in particular, for orchestrating the emergence of long-lived plasma cells3, which continue to secrete antiviral antibodies even when the virus has gone.
[...]
nature.com [2021-07-17] Andreas Radbruch & Hyun-Dong Chang, 14 June 2021 link archive General
A new study has found that individuals that have previously contracted COVID-19 show a more potent antibody response than those who were solely vaccinated for the respiratory virus.
thefederalist.com [2021-08-06] By Shawn Fleetwood, AUGUST 5, 2021 link archive General
The levels of IgG antibodies against SARS-CoV-2 Spike protein remain stable, or even increase, seven months after infection, according to a follow-up study in a cohort of healthcare workers coordinated by the Barcelona Institute for Global Health (ISGlobal), an institution supported by “la Caixa” Foundation, in collaboration with the Hospital Clinic of Barcelona. The results, published in Nature Communications, also support the idea that pre-existing antibodies against common cold coronaviruses could protect against COVID-19.
[...]
scitechdaily.com [2021-08-10] By BARCELONA INSTITUTE FOR GLOBAL HEALTH (ISGLOBAL), AUGUST 6, 2021 link archive General
Most recovered COVID-19 patients mount broad, durable immunity after infection
Neutralizing antibodies show a bi-phasic decay with half-lives >200 days
Spike IgG+ memory B cells increase and persist postinfection
Durable polyfunctional CD4 and CD8 T cells recognize distinct viral epitope regions
cell.com [2021-08-10] Kristen W. Cohen, Susanne L. Linderman, Zoe Moodie, ..., Mehul S. Suthar, Rafi Ahmed, M. Juliana McElrath, July 20, 2021 link archive General
We report broad serological profiles within the cohort, detecting antibody binding to other human coronaviruses. 202(>99%) participants had SARS-CoV-2 specific antibodies, with SARS-CoV-2 neutralization and spike-ACE2 receptor interaction blocking observed in 193(95%) individuals. A significant positive correlation (r=0.7804) between spike-ACE2 blocking antibody titers and neutralization potency was observed. Further, SARS-CoV-2 specific CD8 T-cell responses were clear and quantifiable in 95 of 106(90%) HLA-A2 individuals.
Interpretation
The viral surface spike protein was identified as the dominant target for both neutralizing antibodies and CD8 T-cell responses. Overall, the majority of patients had robust adaptive immune responses, regardless of their disease severity.
thelancet.com [2021-08-10] Stine SF Nielsen, Line K Vibholm, Ida Monrad, Rikke Olesen, Giacomo S Frattari, Marie H Pahus, et al., June 04, 2021 link archive General
It's the 800-pound gorilla in the pandemic. The debate over forced vaccination with an ever-waning vaccine is cresting right around the time when the debate should be moot for a lot of people. Among the most fraudulent messages of the CDC's campaign of deceit is to force the vaccine on those with prior infection, who have a greater degree of protection against all versions of the virus than those with any of the vaccines. It's time to set the record straight once and for all that natural immunity to SARS-CoV-2 is broader, more durable, and longer-lasting than any of the shots on the market today. Our policies must reflect that reality.
theblaze.com [2021-09-02] DANIEL HOROWITZ, August 25, 2021 link archive General
It is unclear why NSP7- and NSP13-specific T cells are detected and often dominant in unexposed donors, while representing a minor population in individuals who have recovered from SARS or COVID-19. It is, however, consistent with the findings of a previous study, in which ORF1-specific T cells were preferentially detected in some donors who were not exposed to SARS-CoV-2 whereas T cells from individuals who had recovered from COVID-19 preferentially recognized structural proteins. Induction of virus-specific T cells in individuals who were exposed but uninfected has been demonstrated in other viral infections. Theoretically, individuals exposed to coronaviruses might just prime ORF1-specific T cells, as the ORF1-encoded proteins are produced first in coronavirus-infected cells and are necessary for the formation of the viral replicase–transcriptase complex that is essential for the subsequent transcription of the viral genome, which then leads to the expression of various RNA species. Therefore, ORF1-specific T cells could hypothetically abort viral production by lysing SARS-CoV-2-infected cells before the formation of mature virions. By contrast, in patients with COVID-19 and SARS, the N protein—which is abundantly produced in cells that secrete mature virions—would be expected to preferentially boost N-specific T cells.
Notably, the ORF1 region contains domains that are highly conserved among many different coronaviruses. The distribution of these viruses in different animal species might result in periodic human contact that induces ORF1-specific T cells with cross-reactive abilities against SARS-CoV-2. Understanding the distribution, frequency and protective capacity of pre-existing structural or non-structural protein-associated SARS-CoV-2 cross-reactive T cells could be important for the explanation of some of the differences in infection rates or pathology observed during this pandemic. T cells that are specific to viral proteins are protective in animal models of airway infections, but the possible effects of pre-existing N- and/or ORF1-specific T cells onthe differential modulation of SARS-CoV-2 infection will have to be carefully evaluated.
nature.com [2021-09-02] Nina Le Bert , ..., Antonio Bertoletti, 15 July 2020 link archive General
Our study demonstrates that convalescent subjects previously infected with ancestral variant SARS-CoV-2 produce antibodies that cross-neutralize emerging VOCs with high potency. Structural and functional analyses reveal that antibody breadth is mediated by targeting a site of vulnerability at the RBD tip offset from major mutational hotspots in VOCs. Selective boosting of immune responses targeting specific RBD epitopes, such as the sites defined by these antibodies, may induce breadth against current and future VOCs.
science.org [2021-09-02] LINGSHU WANG, ..., JOHN MISASI, ..., August 13, 2021 link archive General
We reviewed studies published in PubMed from inception to Sept 28, 2021, and found well conducted biological studies showing protective immunity after infection (panel). Furthermore, multiple epidemiological and clinical studies, including studies during the recent period of predominantly delta (B.1.617.2) variant transmission, found that the risk of repeat SARS-CoV-2 infection decreased by 80·5–100% among those who had had COVID-19 previously (panel). The reported studies were large and conducted throughout the world. Another laboratory-based study that analysed the test results of 9119 people with previous COVID-19 from Dec 1, 2019, to Nov 13, 2020, found that only 0·7% became reinfected.11 In a study conducted at the Cleveland Clinic in Cleveland, OH, USA, those who had not previously been infected had a COVID-19 incidence rate of 4·3 per 100 people, whereas those who had previously been infected had a COVID-19 incidence rate of 0 per 100 people.6 Furthermore, a study conducted in Austria found that the frequency of hospitalisation due to a repeated infection was five per 14 840 (0·03%) people and the frequency of death due to a repeated infection was one per 14 840 (0·01%) people.4 Due to the strong association and biological basis for protection,12 clinicians should consider counselling recovered patients on their risk for reinfection and document previous infection status in medical records.
[...]
thelancet.com [2021-11-18] Noah Kojima ,Jeffrey D Klausner, November 08, 2021 link archive General
We should not force COVID vaccines on anyone when the evidence shows that naturally acquired immunity is equal to or more robust and superior to existing vaccines. Instead, we should respect the right of the bodily integrity of individuals to decide for themselves.
Public health officials and the medical establishment with the help of the politicized media are misleading the public with assertions that the COVID-19 shots provide greater protection than natural immunity. CDC Director Rochelle Walensky, for example, was deceptive in her October 2020 published LANCET statement that “there is no evidence for lasting protective immunity to SARS-CoV-2 following natural infection” and that “the consequence of waning immunity would present a risk to vulnerable populations for the indefinite future.”
Immunology and virology 101 have taught us over a century that natural immunity confers protection against a respiratory virus’s outer coat proteins, and not just one, e.g. the SARS-CoV-2 spike glycoprotein. There is even strong evidence for the persistence of antibodies. Even the CDC recognizes natural immunity for chicken-pox and measles, mumps, and rubella, but not for COVID-19.
[...]
brownstone.org [2021-12-05] BY PAUL ELIAS ALEXANDER, OCTOBER 17, 2021 link archive General
In many countries natural immunity is recognized, at least in some part, as a valid reason to refrain from a COVID vaccine. Here in the U.S., many people facing mandates are unable to use their natural immunity as a justified reason to pass on the vaccine. In fact, it’s almost as if we’d never encountered natural immunity before. Which is odd considering vaccines are developed to mimic the natural immune response.
Several studies, as well as the CDC and other governmental agencies around the world, have come out to say that the immune response induced by the COVID vaccines wanes rather quickly. This is the justification and reason that warrants the need for boosters after just 6 months.
Those who choose to argue that natural immunity may not be suitable, argue that we don’t have long term studies. In fact, we have several studies. Well done studies that indicate that natural immunity is not only robust, but also far superior to the vaccine-induced immune response. So far, as we see vaccine-induced immune responses waning, we’ve yet to see one where natural immunity wanes nearly as quickly.
While we wait for long-term studies on the vaccines to be conducted and reported on, we have these at our fingertips. If the FDA continues to push for 55, and now doubled-down for 75 years to release the data that led them to an EUA approval, we can use this information in the meantime to make an informed decision.
[...]
thewellnessway.com [2022-01-07] Dr. Patrick Flynn, December 20, 2021 link archive General
The Morbidity and Mortality Weekly Report (MMWR) published by the Centers for Disease Control has released a fascinating study on comparing hospitalization with Covid-19 immunity status, thus addressing a topic of pressing concern for public health. The study, published in the January 28, 2022 weekly, carries the self-explanatory title “COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis — California and New York, May–November 2021.”
The key contribution is the following chart, which illustrates the effectiveness of the vaccine (for the duration of the study) and plots that against the effectiveness of natural immunity with and without the vaccine. What it reveals is a point that has been strangely disputed or at least too often left unacknowledged: the power of natural immunity to serve as protection against severe outcomes from reinfection. This reality bears strongly on the question of vaccine mandates.
Natural immunity will be key to downshifting the pandemic to endemic status. That doesn’t mean you should go out and try to catch the virus tomorrow.
In October 2020, a few weeks before the experimental trial results for the BioNTech-Pfizer, Moderna and Oxford/AstraZeneca Covid-19 vaccines were released, German virologist Christian Drosten cautioned that the shots would be of limited effectiveness in preventing the spread of the disease.
“We are dealing here with an infection of the mucous membrane, i.e., in the nose and the throat and then later the lungs,” he said on Episode 62 of Das Coronavirus-Update, the podcast launched by broadcaster NDR in March 2020 that helped make Drosten a household name in Germany. “The mucous membranes already have their own special local immune system. With the current vaccines, which are more likely to be injected into the muscle, you don’t reach this local immune system so well.” As a result, the vaccines “probably protect more against the severe course [of the disease] than against infection.”
Which is of course exactly how things played out. The vaccines have been spectacularly effective at preventing severe disease and death, much less so at preventing transmission.
Drosten has been described in the U.S. media as “Germany’s Fauci,” but the moniker seems a little unfair. National Institute of Allergy and Infectious Diseases Director Anthony Fauci was a top researcher in his day, but has been running a sizable government agency (fiscal year 2021 budget, $6 billion) for the past 38 years. His appearances in the media during the pandemic have mostly involved reciting the public-health consensus of the moment, which was useful when the U.S. president was a font of Covid-19 misinformation but not always especially enlightening. Drosten, director of the Institute of Virology at Berlin’s Charité medical school, is perhaps the world’s leading coronavirus expert, responsible for identifying the original severe acute respiratory syndrome virus in 2003 and devising the first diagnostic test for the Covid-causing SARS-CoV-2 virus in January 2020. His public commentary, delivered chiefly in podcast form after he grew frustrated dealing with some in the German media, has tended toward the cutting-edge and forward-looking — as indicated by what he was saying about vaccines in October 2020.
I recount all this as context for what Drosten said last month in the 113th and final (for now) regular Coronavirus-Update episode. He was talking again about the mucous membrane — which in German is conveyed as the more graphic “Schleimhaut,” literally “slime skin” — and its role in keeping infectious diseases in check (translation and editing-for-brevity by me):
With influenza it is simply the case that everyone gets infected x times over the course of their lives. These infections occur in the mucous membrane, in the throat. Our mucous membranes have a local immune system of their own, if you want to call it that. And everyone in the population, except for the children, of course, has so many infections behind them that there in the mucous membrane, immunity exists. That is why the adults in the population, and that is the vast majority of the population, are not so infectious.
[...]
bloomberg.com [2022-06-02] Justin Fox, April 30, 2022 link archive General
Even I knew (from what I learned in 9th grade and what my mother taught) that the pandemic would only end with endemicity naturally earned. That is precisely what is happening. The CDC’s publication MMWR printed a seroprevalence study showing that from December 2021 to February 2022 – that period during which it seemed like everyone in the country got covid – went from 33.5% to 57.7%. In children, it went from 44.2% to 75.2%. It’s higher in both groups now.
That the study got no real attention to it shows that we are fast moving toward the end, and how? Not through vaccination, which protects against neither infection nor transmission. It ends with everyone meeting the virus. There is of course some threshold of herd immunity with this virus, though it keeps rising with each mutation, requiring ever more rounds of infection to achieve it. It is surely higher than 70% but probably less than 90% depending on population mobility and other factors.
We can look at that data today and wonder. What if we had never locked down? What if we had gone on with life as normally while urging those in risk categories to wait it out a bit while we achieved endemicity? How long would it have taken to get there?
Might it have been over by the summer of 2020? It is possible. It’s hard to know such counterfactuals with precision, but it does seem highly likely that the lockdowns achieved nothing good, caused tremendous damage, and also unnecessarily prolonged the pandemic. In addition, they degraded everyone’s immune system: we didn’t just avoid covid but everything else too.
And the main reason was due to the unwillingness of public health authorities to talk about actual science. When Fauci was asked about natural immunity in September 2021, he said “I don’t have a really firm answer for you on that. That’s something that we’re going to have to discuss regarding the durability of the response…I think that is something that we need to sit down and discuss seriously.”
The WHO even changed its definition of herd immunity to exclude natural infection as a factor! The whole institution gave itself over to vaccine sales based on wild exaggerations of their effectiveness while all-but-denying robust and broad immunity through exposure.
[...]
brownstone.org [2022-06-03] JEFFREY A. TUCKER, JUNE 2, 2022 link archive General
BACKGROUND: The future of the SARS-CoV-2 pandemic hinges on virus evolution and duration of immune protection of natural infection against reinfection. We investigated duration of protection afforded by natural infection, the effect of viral immune evasion on duration of protection, and protection against severe reinfection, in Qatar, between February 28, 2020 and June 5, 2022. METHODS: Three national, matched, retrospective cohort studies were conducted to compare incidence of SARS-CoV-2 infection and COVID-19 severity among unvaccinated persons with a documented SARS-CoV-2 primary infection, to incidence among those infection-naive and unvaccinated. Associations were estimated using Cox proportional-hazard regression models. RESULTS: Effectiveness of pre-Omicron primary infection against pre-Omicron reinfection was 85.5% (95% CI: 84.8-86.2%). Effectiveness peaked at 90.5% (95% CI: 88.4-92.3%) in the 7th month after the primary infection, but waned to ~70% by the 16th month. Extrapolating this waning trend using a Gompertz curve suggested an effectiveness of 50% in the 22nd month and <10% by the 32nd month. Effectiveness of pre-Omicron primary infection against Omicron reinfection was 38.1% (95% CI: 36.3-39.8%) and declined with time since primary infection. A Gompertz curve suggested an effectiveness of <10% by the 15th month. Effectiveness of primary infection against severe, critical, or fatal COVID-19 reinfection was 97.3% (95% CI: 94.9-98.6%), irrespective of the variant of primary infection or reinfection, and with no evidence for waning. Similar results were found in sub-group analyses for those ≥50 years of age. CONCLUSIONS: Protection of natural infection against reinfection wanes and may diminish within a few years. Viral immune evasion accelerates this waning. Protection against severe reinfection remains very strong, with no evidence for waning, irrespective of variant, for over 14 months after primary infection.
medrxiv.org [2022-07-08] (pdf doc) Hiam Chemaitelly, Nico Nagelkerke, Houssein H. Ayoub, ..., Laith J. Abu-Raddad, July 07, 2022 link archive General
Objective: To evaluate dynamics of antibody levels following exposure to SARS-CoV-2 during 12 months in Dutch non-vaccinated hairdressers and hospitality staff.
Methods: In this prospective cohort study, blood samples were collected every three months for one year, and analyzed using a qualitative total antibody ELISA and a quantitative IgG antibody ELISA. Participants filled out questionnaires, providing information on demographics, health and work. Differences in antibody levels were evaluated using Mann-Whitney U and Wilcoxon Signed Rank tests. Beta coefficients (B) and 95% confidence intervals (95%CI) were calculated using linear regression.
Results: Ninety-five of 497 participants (19.1%) had ≥1 seropositive measurement before their last visit using the qualitative ELISA. Only 2.1% (2/95) seroreverted during follow-up. Of the 95 participants, 82 (86.3%) tested IgG seropositive in the quantitative ELISA too. IgG antibody levels significantly decreased in the first months (p<0.01), but remained detectable up to 12 months in all participants. Higher age (B, 10-years increment: 24.6, 95%CI: 5.7-43.5) and higher BMI (B, 5kg/m² increment: 40.0, 95%CI: 2.9-77.2) were significantly associated with a higher peak of antibody levels.
Conclusions: In this cohort, SARS-CoV-2 antibodies persisted for up to one year after initial seropositivity, suggesting long-term natural immunity.
pubmed.ncbi.nlm.nih.gov [2022-12-08] Dymphie Mioch, Leonard Vanbrabant, ..., Sandra Salewicz, November 2022 link archive General
From the beginning of the March 2020 lockdowns for the SARS-CoV-2 virus, the subject of natural immunity (also called post-infection immunity) has been neglected. Once the vaccination became widely available, what began with near silence at the beginning turned nearly into a complete blackout of the topic.
Even now, there is an absence of open discussion, presumably in the interests of promoting universal vaccination and required documentation of such vaccination as a condition of participating in public life and even the jobs marketplace. Still, the science exists. Many studies exist. Their authors deserve credit, recognition, and to have their voices heard.
These studies demonstrate what was and is already known: natural immunity for a SARS-type virus is robust, long-lasting, and broadly effective even in the case of mutations, generally more so than vaccines. In fact, a major contribution of 20th-century science has been to expand upon and further elucidate this principle that has been known since the ancient world. Every expert presumably knew this long before the current debates. The effort to pretend otherwise is a scientific scandal of the highest order, especially because the continued neglect of the topic is affecting the rights and freedoms of billions of people.
[...]
brownstone.org [2022-12-12] Brownstone Institute, October 10, 2021 link archive General
We should not force COVID vaccines on anyone when the evidence shows that naturally acquired immunity is equal to or more robust and superior to existing vaccines. Instead, we should respect the right of the bodily integrity of individuals to decide for themselves.
Public health officials and the medical establishment with the help of the politicized media are misleading the public with assertions that the COVID-19 shots provide greater protection than natural immunity. CDC Director Rochelle Walensky, for example, was deceptive in her October 2020 published LANCET statement that “there is no evidence for lasting protective immunity to SARS-CoV-2 following natural infection” and that “the consequence of waning immunity would present a risk to vulnerable populations for the indefinite future.”
Immunology and virology 101 have taught us over a century that natural immunity confers protection against a respiratory virus’s outer coat proteins, and not just one, e.g. the SARS-CoV-2 spike glycoprotein. There is even strong evidence for the persistence of antibodies. Even the CDC recognizes natural immunity for chicken-pox and measles, mumps, and rubella, but not for COVID-19.
The vaccinated are showing viral loads (very high) similar to the unvaccinated (Acharya et al. and Riemersma et al.), and the vaccinated are as infectious. Riemersma et al. also report Wisconsin data that corroborate how the vaccinated individuals who get infected with the Delta variant can potentially (and are) transmit(ting) SARS-CoV-2 to others (potentially to the vaccinated and unvaccinated).
This troubling situation of the vaccinated being infectious and transmitting the virus emerged in seminal nosocomial outbreak papers by Chau et al. (HCWs in Vietnam), the Finland hospital outbreak (spread among HCWs and patients), and the Israel hospital outbreak (spread among HCWs and patients). These studies also revealed that the PPE and masks were essentially ineffective in the healthcare setting. Again, the Marek’s disease in chickens and the vaccination situation explains what we are potentially facing with these leaky vaccines (increased transmission, faster transmission, and more ‘hotter’ variants).
This follow-up chart is the most updated and comprehensive library list of 150 of the highest-quality, complete, most robust scientific studies and evidence reports/position statements on natural immunity as compared to the COVID-19 vaccine-induced immunity and allow you to draw your own conclusion.
[...]
brownstone.org [2022-12-12] Paul Elias Alexander, October 17, 2021 link archive General
Understanding the level and characteristics of protection from past SARS-CoV-2 infection against subsequent re-infection, symptomatic COVID-19 disease, and severe disease is essential for predicting future potential disease burden, for designing policies that restrict travel or access to venues where there is a high risk of transmission, and for informing choices about when to receive vaccine doses. We aimed to systematically synthesise studies to estimate protection from past infection by variant, and where data allow, by time since infection.
Methods
In this systematic review and meta-analysis, we identified, reviewed, and extracted from the scientific literature retrospective and prospective cohort studies and test-negative case-control studies published from inception up to Sept 31, 2022, that estimated the reduction in risk of COVID-19 among individuals with a past SARS-CoV-2 infection in comparison to those without a previous infection. We meta-analysed the effectiveness of past infection by outcome (infection, symptomatic disease, and severe disease), variant, and time since infection. We ran a Bayesian meta-regression to estimate the pooled estimates of protection. Risk-of-bias assessment was evaluated using the National Institutes of Health quality-assessment tools. The systematic review was PRISMA compliant and was registered with PROSPERO (number CRD42022303850).
Findings
We identified a total of 65 studies from 19 different countries. Our meta-analyses showed that protection from past infection and any symptomatic disease was high for ancestral, alpha, beta, and delta variants, but was substantially lower for the omicron BA.1 variant. Pooled effectiveness against re-infection by the omicron BA.1 variant was 45·3% (95% uncertainty interval [UI] 17·3–76·1) and 44·0% (26·5–65·0) against omicron BA.1 symptomatic disease. Mean pooled effectiveness was greater than 78% against severe disease (hospitalisation and death) for all variants, including omicron BA.1. Protection from re-infection from ancestral, alpha, and delta variants declined over time but remained at 78·6% (49·8–93·6) at 40 weeks. Protection against re-infection by the omicron BA.1 variant declined more rapidly and was estimated at 36·1% (24·4–51·3) at 40 weeks. On the other hand, protection against severe disease remained high for all variants, with 90·2% (69·7–97·5) for ancestral, alpha, and delta variants, and 88·9% (84·7–90·9) for omicron BA.1 at 40 weeks.
Interpretation
Protection from past infection against re-infection from pre-omicron variants was very high and remained high even after 40 weeks. Protection was substantially lower for the omicron BA.1 variant and declined more rapidly over time than protection against previous variants. Protection from severe disease was high for all variants. The immunity conferred by past infection should be weighed alongside protection from vaccination when assessing future disease burden from COVID-19, providing guidance on when individuals should be vaccinated, and designing policies that mandate vaccination for workers or restrict access, on the basis of immune status, to settings where the risk of transmission is high, such as travel and high-occupancy indoor settings.
thelancet.com [2023-02-28] Caroline Stein, Hasan Nassereldine, ..., Stephen S Lim, February 16, 2023 link archive General
It has long been hypothesized that attractiveness provides a cue to a target's health and immunocompetence. However, much of the research testing this hypothesis has relied on a small number of indirect proxies of immune function, and the results of this research have been mixed. Here, we build on this past research, examining the relationship between target attractiveness and (i) self-reported health, (ii) in vivo measures of inflammation and white blood cell count/composition, and (iii) in vitro tests of targets' immune function, including (c1) leucocyte proliferation in response to immunological stimulants, (c2) phagocytosis of Escherichia coli bioparticles, (c3) NK cell-mediated lysis of target tumour cells, and (c4) Staphylococcus aureus growth in isolated plasma. Results revealed multiple, sometimes sex-differentiated, relationships between targets' immune function and others’ perceptions of their attractiveness. Together, this work suggests complex, often sex-differentiated relationships between immune function, health, and attractiveness.
[...]
6. Conclusion
Researchers have long speculated that perceptions of attractiveness reflect preferences for traits historically linked to health and, ultimately, immune function (e.g. [6]). The results of the current research suggest that facial attractiveness may provide insights into one's immune function, particularly as it relates to one's ability to efficiently combat (primarily) bacterial threats. Additionally, for men, facial attractiveness may also provide cues to their ability to efficiently manage viral threats and neoplastic growth. Although future research is needed replicate these results, the current research suggests that a relationship between facial attractiveness and immune function is likely to exist.
[...]
royalsocietypublishing.org [2022-02-21] Summer Mengelkoch, Jeff Gassen, Marjorie L. Prokosch, Gary W. Boehm, Sarah E. Hill, 16 February 2022 link archive General
- Testing (PCR/Antibody) -
More information on PCR Testing
More information on COVID-19 Rapid Antigen Test
More information on COVID-19 Antibody / Serology Tests
1) COVID-19 Infections (Infections due to SARS-CoV-2)
a) Code only confirmed cases Code only a confirmed diagnosis of the 2019 novel coronavirus disease (COVID-19) as documented by the provider, documentation of a positive COVID-19 test result, or a presumptive positive COVID-19 test result. For a confirmed diagnosis, assign code U07.1, COVID-19. This is an exception to the hospital inpatient guideline Section II, H. In this context, “confirmation” does not require documentation of the type of test performed; the provider’s documentation that the individual has COVID-19 is sufficient.
Presumptive positive COVID-19 test results should be coded as confirmed. A presumptive positive test result means an individual has tested positive for the virus at a local or state level, but it has not yet been confirmed by the Centers for Disease Control and Prevention (CDC). CDC confirmation of local and state tests for COVID-19 is no longer required.
If the provider documents "suspected," "possible," "probable," or “inconclusive” COVID19, do not assign code U07.1. Assign a code(s) explaining the reason for encounter (such as fever) or Z20.828, Contact with and (suspected) exposure to other viral communicable diseases.
[...]
cdc.gov [2021-09-02] (pdf doc) April 1, 2020; through September 30, 2020 link archive General
- The COVID-19 disease - PCR testing process and its inability to identify a virus - Naturally occurring exosomes, how they're induced and their relation to virus bodies - Overview of some treatments
youtube.com [2020-06-04] Secrets of Saturn channel Mar 30, 2020 link archive General
Testing for SARS-CoV-2 is central to COVID-19 management and has relied on quantitative reverse transcriptase polymerase chain reaction (PCR) technology. PCR seeks the genetic code of the virus from nose or throat swabs and amplifies it over 30–40 cycles, doubling each cycle, enabling even miniscule, potentially single, copies to be detected. PCR is thus a powerful clinical test, specifically when a patient is, or was recently, infected with SARS-CoV-2. Fragments of RNA can linger for weeks after infectious virus has been cleared, often in people without symptoms or known exposures.
However, for public health measures, another approach is needed. Testing to help slow the spread of SARS-CoV-2 asks not whether someone has RNA in their nose from earlier infection, but whether they are infectious today. It is a net loss to the health, social, and economic wellbeing of communities if post-infectious individuals test positive and isolate for 10 days. In our view, current PCR testing is therefore not the appropriate gold standard for evaluating a SARS-CoV-2 public health test.
Most people infected with SARS-CoV-2 are contagious for 4–8 days. Specimens are generally not found to contain culture-positive (potentially contagious) virus beyond day 9 after the onset of symptoms, with most transmission occurring before day 5. This timing fits with the observed patterns of virus transmission (usually 2 days before to 5 days after symptom onset), which led public health agencies to recommend a 10-day isolation period. The short window of transmissibility contrasts with a median 22–33 days of PCR positivity (longer with severe infections and somewhat shorter among asymptomatic individuals). This suggests that 50–75% of the time an individual is PCR positive, they are likely to be post-infectious.
[Emphasis added. See link for footnotes.]
thelancet.com [2021-03-21] Michael J Mina, Tim E Peto, Marta García-Fiñana, Malcolm G Semple, Iain E Buchan, Published: February 17, 2021 link archive General
ITALY: Scientists use lateral flow antigen rapid "SARSCoV2 test" on a kiwi fruit. The kiwi fruit is positive. Please note: there are no tests for Covid19. Selling these as "tests" is a global fraud.
[...]
What is the solution?
1. Stop ALL asymptomatic mass testing immediately as a matter of urgency. Refuse to be tested.
ORLANDO, Fla. - After FOX 35 News noticed errors in the state's report on positivity rates, the Florida Department of Health said that some laboratories have not been reporting negative test result data to the state.
Countless labs have reported a 100 percent positivity rate, which means every single person tested was positive. Other labs had very high positivity rates. FOX 35 News found that testing sites like one local Centra Care reported that 83 people were tested and all tested positive. Then, NCF Diagnostics in Alachua reported 88 percent of tests were positive.
[...]
The report showed that Orlando Health had a 98 percent positivity rate. However, when FOX 35 News contacted the hospital, they confirmed errors in the report. Orlando Health's positivity rate is only 9.4 percent, not 98 percent as in the report.
The report also showed that the Orlando Veteran’s Medical Center had a positivity rate of 76 percent. A spokesperson for the VA told FOX 35 News on Tuesday that this does not reflect their numbers and that the positivity rate for the center is actually 6 percent.
fox35orlando.com [2020-07-15] By Robert Guaderrama, July 14, 2020 link archive General
It’s also unclear to what extent people with no symptoms transmit SARS-CoV-2. The only test for live virus is viral culture. PCR and lateral flow tests do not distinguish live virus. No test of infection or infectiousness is currently available for routine use.678 As things stand, a person who tests positive with any kind of test may or may not have an active infection with live virus, and may or may not be infectious.9
The Centers for Disease Control and Prevention (CDC) acknowledged Thursday that it is combining the results from viral and antibody COVID-19 tests when reporting the country's testing totals, despite marked differences between the tests.
[...]
Viral tests — commonly referred to as PCR tests as most of them use a process known as polymerase chain reaction — are used by health professionals to determine whether or not a person is currently infected with the disease. During the pandemic, viral tests have been the most effective way of being able to diagnose a positive case of COVID-19. They are what state governments have been counting to track the number of confirmed cases of the virus they have.
Antibody, or serology, tests serve a different purpose. Unlike viral tests that are taken by nose swab or saliva sample, antibody tests examine a person's blood to see if their immune system has created antibodies to combat COVID-19. These tests allow doctors to see if someone has previously been exposed to the virus. As the push for widespread testing in the U.S. has strengthened, antibody tests have been widely produced, many experts have balked at saying that antibodies equate to immunity from COVID-19. Serology tests are also less accurate than PCR tests, increasing the chances for a false negative.
thehill.com [2020-06-30] BY MARTY JOHNSON, 05/21/20 link archive General
For anyone willing to look, there are so many facts that tell the true story, and it goes something like this:
Knowing what we know today about COVID-19’s Infection Fatality Rate, asymmetric impact by age and medical condition, non-transmissibility by asymptomatic people and in outdoor settings, near-zero fatality rate for children, and the basic understanding of viruses through Farr’s law, locking down society was a bone-headed policy decision so devastating to society that historians may judge it as the all-time worst decision ever made. Worse, as these clear facts have become available, many policy-makers haven’t shifted their positions, despite the fact that every hour under any stage of lockdown has a domino-effect of devastation to society. Meanwhile, the media—with a few notable exceptions—is oddly silent on all the good news. Luckily, an unexpected group of heroes across the political landscape—many of them doctors and scientists—have emerged to tell the truth, despite facing extreme criticism and censorship from an angry mob desperate to continue fighting an imaginary war.
Fact #1: The Infection Fatality Rate for COVID-19 is somewhere between 0.07-0.20%, in line with seasonal flu
Fact #2: The risk of dying from COVID-19 is much higher than the average IFR for older people and those with co-morbidities, and much lower than the average IFR for younger healthy people, and nearing zero for children
Fact #3: People infected with COVID-19 who are asymptomatic (which is most people) do NOT spread COVID-19
Fact #4: Emerging science shows no spread of COVID-19 in the community (shopping, restaurants, barbers, etc.)
Fact #5: Published science shows COVID-19 is NOT spread outdoors
Fact #6: Science shows masks are ineffective to halt the spread of COVID-19, and The WHO recommends they should only be worn by healthy people if treating or living with someone with a COVID-19 infection
Fact #7: There’s no science to support the magic of a six-foot barrier
Fact #8: The idea of locking down an entire society had never been done and has no supportable science, only theoretical modeling
Fact #9: The epidemic models of COVID-19 have been disastrously wrong, and both the people and the practice of modeling has a terrible history
Fact #10: The data shows that lockdowns have NOT had an impact on the course of the disease.
Fact #11: Florida locked down late, opened early, and is doing fine, despite predictions of doom
Fact #12: New York’s above average death rate appears to be driven by a fatal policy error combined with aggressive intubations.
Fact #13: Public health officials and disease epidemiologists do NOT consider the other negative societal consequences of lockdowns
Fact #14: There is a predictive model for the viral arc of COVID-19, it’s called Farr’s Law, and it was discovered over 100 years ago
Fact #15: The lockdowns will cause more death and destruction than COVID-19 ever did
Fact #16: All these phased re-openings are utter nonsense with no science to support them, but they will all be declared a success
thewallwillfall.org By J.B. Handley, June 5, 2020 link archive General
The Centers for Disease Control and Prevention, no longer restricted by the Trump administration, issued an extensive federal public health order late Friday requiring all individuals to wear masks over their mouth and nose on nearly all forms of public transportation and private ride-sharing services—and makes refusal to wear a face-covering a violation of federal law.
forbes.com [2021-01-31] Tommy Beer, Jan 30, 2021 link archive General
Jay Bhattacharya, a professor of medicine, told The Telegraph's Planet Normal podcast, which you can listen to using the audio player above, that there have been "enormous collateral consequences" of keeping people inside and isolating them from their loved-ones during the Covid-19 pandemic.
The epidemiologist believes many scientists have clung onto the perceived effectiveness of lockdowns, and they "remain attached" to the idea despite the "failure of this strategy".
"I do think that future historians will look back on this and say this was the single biggest public health mistake, possibly of all history, in terms of the scope of the harm that it's caused," said Prof Bhattacharya.
telegraph.co.uk [2021-06-17] June 10, 2021 link archive General
The impact of COVID-19 on the physical health of the world's citizens is extraordinary. By mid-May there were upward of four million cases spread across more than 180 countries. The pandemic's effect on mental health could be even more far-reaching. At one point roughly one third of the planet's population was under orders to stay home. That means 2.6 billion people--more than were alive during World War II--were experiencing the emotional and financial reverberations of this new coronavirus. "[The lockdown] is arguably the largest psychological experiment ever conducted," wrote health psychologist Elke Van Hoof of Free University of Brussels-VUB in Belgium. The results of this unwitting experiment are only beginning to be calculated.
scientificamerican.com [2021-06-17] By Lydia Denworth, June 6, 2020 link archive General
New Zealand entered a strict three-day national lockdown Tuesday after a single case of coronavirus was detected in Auckland, the first locally transmitted example in six months.
The last community outbreak in the South Pacific nation was in February and New Zealand has reported just 26 virus deaths nationally since the pandemic began.
Despite that virus-free stretch, Prime Minister Jacinda Ardern confirmed she would move to Alert Level Four on the presumption the Delta variant has been isolated, saying it was important for the country to “go hard and go early.”
Level Four means reducing contact between people to the bare, essential minimum with the closing of schools, offices and all businesses with only essential services remaining operational.
“As we’ve seen overseas, particularly in Sydney, unnecessary trips outdoors can spread the virus,” the former president of the International Union of Socialist Youth said. (see below)
breitbart.com [2021-08-18] SIMON KENT, 17 Aug 2021 link archive General
New South Wales (NSW) Premier Gladys Berejiklian said on Monday that seven people had died of Covid-19 in the past 24 hours. It is the highest number of related deaths in the region since the pandemic started.
Some 478 new positive cases were reported in NSW on Monday – the highest daily figure since the pandemic began. Sydney has entered its eighth week of lockdown, which is being enforced not only by the Australian police, but also the military.
Australia has now recorded 55 Covid deaths since July 11, and 966 deaths since the emergence of the coronavirus.
Among the seven dead on Monday was a 15-year-old boy from Sydney, who also had pneumococcal meningitis.
More information on Global COVID-19 Quarantine Measures
Face Masks / PPE Controversy
Pease refer to section on Coronavirus Masks / Personal Protection Equipment
- Treatments / Therapy -
Official health institutions, philanthropic organizations, main-stream media outlets and even international corporations are pushing vaccines as the most important treatment for the prevention of COVID-19. See more information on Coronavirus vaccines and their efficacy and safety.
However, many doctors have spoken out regarding alternative treatments. In several cases, these doctors have been censored and therefore much of the public is unaware of other treatments and preventative measures that can be taken to protect against COVID-19. See more information on COVID-19 Prophylaxis & Treatment Alternatives
More information on Hospital protocols & standard treatments for COVID-19 patients
The Administration is taking aggressive actions and exercising regulatory flexibilities to help healthcare providers contain the spread of 2019 Novel Coronavirus Disease (COVID-19). CMS is empowered to take proactive steps through 1135 waivers as well as, where applicable, authority granted under section 1812(f) of the Social Security Act (the Act) and rapidly expand the Administration’s aggressive efforts against COVID-19. As a result, the following blanket waivers are in effect, with a retroactive effective date of March 1, 2020, through the end of the emergency declaration. For general information about waivers, see Attachment A to this document. These waivers DO NOT require a request to be sent to the 1135waiver@cms.hhs.gov mailbox or that notification be made to any of CMS’ regional offices.
Unless otherwise noted, these waivers will terminate at the end of the COVID-19 public health emergency (PHE).
[...]
cms.gov [2023-02-11] (pdf doc) Centers for Medicare and Medicaid Services link archive General
Under President Trump’s leadership, the Centers for Medicare & Medicaid Services (CMS) has broadened access to Medicare telehealth services so that beneficiaries can receive a wider range of services from their doctors without having to travel to a healthcare facility. These policy changes build on the regulatory flexibilities granted under the President’s emergency declaration. CMS is expanding this benefit on a temporary and emergency basis under the 1135 waiver authority and Coronavirus Preparedness and Response Supplemental Appropriations Act. The benefits are part of the broader effort by CMS and the White House Task Force to ensure that all Americans – particularly those at high-risk of complications from the virus that causes the disease COVID-19 – are aware of easy-to-use, accessible benefits that can help keep them healthy while helping to contain the community spread of this virus.
[...]
MEDICARE TELEHEALTH VISITS: Currently, Medicare patients may use telecommunication technology for office, hospital visits and other services that generally occur in-person.
The provider must use an interactive audio and video telecommunications system that permits real-time communication between the distant site and the patient at home. Distant site practitioners who can furnish and get payment for covered telehealth services (subject to state law) can include physicians, nurse practitioners, physician assistants, nurse midwives, certified nurse anesthetists, clinical psychologists, clinical social workers, registered dietitians, and nutrition professionals.
It is imperative during this public health emergency that patients avoid travel, when possible, to physicians’ offices, clinics, hospitals, or other health care facilities where they could risk their own or others’ exposure to further illness. Accordingly, the Department of Health and Human Services (HHS) is announcing a policy of enforcement discretion for Medicare telehealth services furnished pursuant to the waiver under section 1135(b)(8) of the Act. To the extent the waiver (section 1135(g)(3)) requires that the patient have a prior established relationship with a particular practitioner, HHS will not conduct audits to ensure that such a prior relationship existed for claims submitted during this public health emergency.
[...]
cms.gov [2023-02-11] Telehealth, Mar 17, 2020 link archive General
Politics in the Corona crisis did not come out of the blue. The “fight against viruses” began as early as the 1990s as the “fight against bioterror”. Research shows that for more than twenty years, pandemic scenarios have been repeatedly rehearsed in business games, first in the USA and later internationally, also with German participation. The titles of these exercises are reminiscent of Hollywood productions: "Dark Winter" (2001), "Global Mercury" (2003), "Atlantic Storm" (2005) or "Clade X" (2018). High-ranking officials and government representatives as well as well-known journalists were involved, most recently, at "Event 201" in October 2019, also board members of large global corporations. After the World Health Organization (WHO) declared a coronavirus pandemic in 2020, many of the measures that had been tried and discussed for years were implemented globally.
Passages like this appeared in the scripts 20 years ago: “The sight of armed military presence in American cities provokes protests against the curtailment of civil liberties (...) The question is how and to what extent we enforce these things. How much force do you use to keep people in their homes?” In the event of a pandemic, “basic civil rights like the right to assemble or the right to travel could no longer be taken for granted.” Restrictions on freedom, but also mass vaccinations, were a regular part of the simulation games.
This lecture will trace chronologically how these exercises came about, who organized them and what parallels the scripts have with the current situation. Is the virus just a pretext for a long-planned global transformation? And was a severe stock market tremor in September 2019 perhaps the actual trigger for the global lockdown?
Chapter overview:
0:00:00 Pandemic business games - preparing for a new era?
0:02:23 The Cold War era 1945 - 1990
0:05:05 The US is running out of enemies
0:17:05 Bioterror simulation games 1990 - 2005
0:23:51 The “Dark Winter” exercise
0:30:44 Contingency planning for bioterror and flu pandemics
0:35:40 Interim conclusion
0:38:40 The “Lock Step Scenario” 2010
0:44:38 “MARS” and The G20 Health Ministers Meeting in Berlin
0:50:35 Why the Corona pandemic started in 2020
0:58:19 Event 201 - Practicing with a coronavirus pandemic
The lecture was recorded on November 20th, 2020 in Berlin.
bitchute.com [2022-01-13] Tell Me Sweet Little Lies channel, May 26th, 2021 link archive General
An exclusive group of thought leaders gathered at the museum to discuss how the world prepares for the next global pandemic, raises public awareness, and explores potential responses and solutions
youtube.com [2022-01-13] Smithsonian Magazine channel, November 14, 2017 link archive General
Operation Dark Winter was the code name for a senior-level bio-terrorist attack simulation conducted from June 22–23, 2001. It was designed to carry out a mock version of a covert and widespread smallpox attack on the United States. Tara O'Toole and Thomas Inglesby of the Johns Hopkins Center for Civilian Biodefense Strategies (CCBS) / Center for Strategic and International Studies (CSIS), and Randy Larsen and Mark DeMier of Analytic Services were the principal designers, authors, and controllers of the Dark Winter project.
The Rockefeller Foundation believes that in order to understand the many ways in which technology will impact international development in the future, we must first broaden
and deepen our individual and collective understanding of the range of possibilities.
THE SCENARIO NARRATIVES . . .
Lock Step
A world of tighter top-down government control and more authoritarian eadership, with limited innovation and growing citizen pushback
Clever Together
A world in which highly coordinated and successful strategies emerge for addressing both urgent and entrenched worldwide issues
Hack Attack
An economically unstable and shock-prone world in which governments weaken, criminals thrive, and dangerous innovations emerge
Smart Scramble
An economically depressed world in which individuals and communities develop localized, makeshift solutions to a growing set of problems
www.nommeraadio.ee via archive.org (WayBackMachine) (pdf doc) May 2010 link archive Simulations/Exercises
More information on Lock Step, a pre-planned reaction to a global pandemic, outlined in the Rockefeller-supported "Scenarios for the Future of Technology and International Development."
The following narrative comprises a futuristic scenario that illustrates communication dilemmas concerning medical countermeasures (MCMs) that could plausibly emerge in the not-so-distant future. Its purpose is to prompt users, both individually and in discussion with others, to imagine the dynamic and oftentimes conflicted circumstances in which communication around emergency MCM development, distribution, and uptake takes place. While engaged with a rigorous simulated health emergency, scenario readers have the opportunity to mentally “rehearse” responses while also weighing the implications of their actions. At the same time, readers have a chance to consider what potential measures implemented in today’s environment might avert comparable communication dilemmas or classes of dilemmas in the future.
[...]
jhsphcenterforhealthsecurity.s3.amazonaws.com [2021-12-18] (pdf doc) Johns Hopkins Center for Health Security, Monica Schoch-Spana, Matthew P. Shearer, ..., Gigi Kwik Gronvall, October 2017 link archive General
Event 201 was a 3.5-hour pandemic tabletop exercise that simulated a series of dramatic, scenario-based facilitated discussions, confronting difficult, true-to-life dilemmas associated with response to a hypothetical, but scientifically plausible, pandemic. 15 global business, government, and public health leaders were players in the simulation exercise that highlighted unresolved real-world policy and economic issues that could be solved with sufficient political will, financial investment, and attention now and in the future.
The exercise consisted of pre-recorded news broadcasts, live “staff” briefings, and moderated discussions on specific topics. These issues were carefully designed in a compelling narrative that educated the participants and the audience.
The Johns Hopkins Center for Health Security, World Economic Forum, and Bill & Melinda Gates Foundation jointly propose these recommendations.
centerforhealthsecurity.org link archive Simulations/Exercises
COVID-19 threatens to become one of the most difficult tests faced by humanity in modern history. As the pandemic has spread it has taken lives, stirred anxiety and political drama, overwhelmed health systems, and triggered potentially lasting geopolitical change. The International Monetary Fund says the global economy now faces its worst downturn since the Great Depression, and Oxfam International has warned that half a billion people could be pushed into poverty as a result of the unfolding crisis. Around the world, desperate efforts are underway to contain what has become a profoundly disruptive outbreak.
This Act may be cited as the ``Coronavirus Aid, Relief, and Economic
Security Act'' or the ``CARES Act''.
[...]
TITLE V--CORONAVIRUS RELIEF FUNDS
Sec. 5001. Coronavirus Relief Fund.
TITLE VI--MISCELLANEOUS PROVISIONS
Sec. 6001. COVID-19 borrowing authority for the United States Postal
Service.
Sec. 6002. Emergency designation.
DIVISION B--EMERGENCY APPROPRIATIONS FOR CORONAVIRUS HEALTH RESPONSE AND
AGENCY OPERATIONS
[...]
congress.gov [2022-01-11] Modified: 03/27/2020, Became Public Law No: 116-136. link archive General
WASHINGTON -- Nearly 1.1 million coronavirus relief payments totaling some $1.4 billion went to dead people, a government watchdog reported Thursday. Legal and political issues hang over the misdirected taxpayer funds, the latest example of errors in massive aid being dispensed at crisis speed.
More than 130 million so-called economic impact payments were sent to taxpayers as part of the $2.4 trillion coronavirus relief package enacted in March. The Government Accountability Office, Congress' auditing arm, cited the number of erroneous payments to deceased taxpayers in its report on the government programs.
[...]
abcnews.go.com [2022-01-11] By MARCY GORDON, AP, 26 June 2020 link archive General
To authorize the Secretary of Health and Human Services to award grants to eligible entities to conduct diagnostic testing for COVID–19, and related activities such as contact tracing, through mobile health units and, as necessary, at individuals’ residences, and for other purposes.
This bill would provide $100 billion in grants to faith-based organization, clinics, medical centers, and other organization which perform testing for COVID–19, tracing of exposure to COVID–19, or services for individuals who are isolating at home. The funding could be used to pay their staff or purchase personal protective equipment to protect their staff.
No provision in this bill would make testing or quarantining mandatory. The bill includes privacy protections for the medical information of individuals that would limit how grantee organizations could share information collected with the federal government. (A widely seen disinformation campaign has made absurd claims about this bill.)
[HR 6666 does not REQUIRE the vaccination of the population as some entities have falsely claimed. However, the bill does provide 100 billion dollars for fiscal year 2020 and further sums as necessary for 2021 and beyond for COVID-19 testing and contact tracing.]
The Secretary is issuing this Declaration pursuant to section 319F-3 of the Public Health Service Act to provide liability immunity for activities related to medical countermeasures against COVID-19.
[...]
Section XIV. Countermeasures Injury Compensation Program
Section 319F-4 of the PHS Act, 42 U.S.C. 247d-6e, authorizes the Countermeasures Injury Compensation Program (CICP) to provide benefits to eligible individuals who sustain a serious physical injury or die as a direct result of the administration or use of a Covered Countermeasure. Compensation under the CICP for an injury directly caused by a Covered Countermeasure is based on the requirements set forth in this Declaration, the administrative rules for the Program, and the statute. To show direct causation between a Covered Countermeasure and a serious physical injury, the statute requires “compelling, reliable, valid, medical and scientific evidence.” The administrative rules for the Program further explain the necessary requirements for eligibility under the CICP. Please note that, by statute, requirements for compensation under the CICP may not align with the requirements for liability immunity provided under the PREP Act. Section XIV of the Declaration, “Countermeasures Injury Compensation Program,” explains the types of injury and standard of evidence needed to be considered for compensation under the CICP.
federalregister.gov [2020-09-21] A Notice by the Health and Human Services Department on 03/17/2020 link archive General
TITLE III—GENERAL POWERS AND DUTIES OF PUBLIC HEALTH SERVICE
DATA COLLECTION REGARDING PROGRAMS UNDER TITLE XXVI SEC.
318B. ø247c–2¿ For the purpose of collecting and providing data for program planning and evaluation activities under title XXVI, there are authorized to be appropriated to the Secretary (acting through the Director of the Centers for Disease Control and Prevention) such sums as may be necessary for each of the fiscal years 2001 through 2005. Such authorization of appropriations is in addition to other authorizations of appropriations that are available for such purpose.
SEC. 319. ø247d¿ PUBLIC HEALTH EMERGENCIES.
(a) EMERGENCIES.—If the Secretary determines, after consultation with such public health officials as may be necessary, that— (1) a disease or disorder presents a public health emergency; or (2) a public health emergency, including significant outbreaks of infectious diseases or bioterrorist attacks, otherwise exists, the Secretary may take such action as may be appropriate to respond to the public health emergency, including making grants, providing awards for expenses, and entering into contracts and conducting and supporting investigations into the cause, treatment, or prevention of a disease or disorder as described in paragraphs (1) and (2). Any such determination of a public health emergency terminates upon the Secretary declaring that the emergency no longer exists, or upon the expiration of the 90-day period beginning on the date on which the determination is made by the Secretary, whichever occurs first. Determinations that terminate under the preceding sentence may be renewed by the Secretary (on the basis of the same or additional facts), and the preceding sentence applies to each such renewal. Not later than 48 hours after making a determination under this subsection of a public health emergency (including a renewal), the Secretary shall submit to the Congress written notification of the determination.
(b) PUBLIC HEALTH EMERGENCY FUND.—
(1) IN GENERAL.—There is established in the Treasury a fund to be designated as the ‘‘Public Health Emergency Fund’’ to be made available to the Secretary without fiscal year limitation to carry out subsection (a) only if a public health emergency has been declared by the Secretary under such subsection or if the Secretary determines there is the significant potential for a public health emergency, to allow the Secretary to rapidly respond to the immediate needs resulting from such public health emergency or potential public health emergency. The Secretary shall plan for the expedited distribution of funds to appropriate agencies and entities. There is authorized to be appropriated to the Fund such sums as may be necessary. (2) USES.—The Secretary may use amounts in the Fund established under paragraph (1), to—
[...]
(C) facilitate and accelerate, as applicable, advanced research and development of security countermeasures (as defined in section 319F–2), qualified countermeasures (as defined in section 319F–1), or qualified pandemic or epidemic products (as defined in section 319F–3), that are applicable to the public health emergency or potential public health emergency under paragraph (1);
[...]
govinfo.gov [2021-07-17] (pdf doc) Enacted: May 26, 2021 link archive General
PRESIDENT BIDEN’S PLAN TO PROVIDE DIRECT RELIEF TO AMERICANS, CONTAIN COVID-19, AND RESCUE THE ECONOMY
The American Rescue Plan is delivering direct relief to the American people, rescuing the American economy, and starting to beat the virus. For a full overview of what’s in the plan, click here.
SEC. 313. <> PUBLIC AWARENESS CAMPAIGN ON THE IMPORTANCE OF VACCINATIONS.
(a) <> In General.--The Secretary, acting through the Director of the Centers for Disease Control and Prevention and in coordination with other offices and agencies, as appropriate, shall award competitive grants or contracts to one or more public or private entities to carry out a national, evidence-based campaign to increase awareness and knowledge of the safety and effectiveness of vaccines for the prevention and control of diseases, combat misinformation about vaccines, and disseminate scientific and evidence-based vaccine-related information, with the goal of increasing rates of vaccination across all ages, as applicable, particularly in communities with low rates of vaccination, to reduce and eliminate vaccine-preventable diseases.
[...]
congress.gov [2022-03-19] 12/27/2020 Became Public Law No: 116-260. link archive General
§245. Public awareness campaign on the importance of vaccinations
(a) In general
The Secretary, acting through the Director of the Centers for Disease Control and Prevention and in coordination with other offices and agencies, as appropriate, shall award competitive grants or contracts to one or more public or private entities to carry out a national, evidence-based campaign to increase awareness and knowledge of the safety and effectiveness of vaccines for the prevention and control of diseases, combat misinformation about vaccines, and disseminate scientific and evidence-based vaccine-related information, with the goal of increasing rates of vaccination across all ages, as applicable, particularly in communities with low rates of vaccination, to reduce and eliminate vaccine-preventable diseases.
(b) Consultation
In carrying out the campaign under this section, the Secretary shall consult with appropriate public health and medical experts, including the National Academy of Medicine and medical and public health associations and nonprofit organizations, in the development, implementation, and evaluation of the evidence-based public awareness campaign.
(c) Requirements
The campaign under this section shall-
(1) be a nationwide, evidence-based media and public engagement initiative;
(2) include the development of resources for communities with low rates of vaccination, including culturally and linguistically appropriate resources, as applicable;
(3) include the dissemination of vaccine information and communication resources to public health departments, health care providers, and health care facilities, including such providers and facilities that provide prenatal and pediatric care;
(4) be complementary to, and coordinated with, any other Federal, State, local, or Tribal efforts, as appropriate; and
(5) assess the effectiveness of communication strategies to increase rates of vaccination.
(d) Additional activities
The campaign under this section may-
(1) include the use of television, radio, the internet, and other media and telecommunications technologies;
(2) include the use of in-person activities;
(3) be focused to address specific needs of communities and populations with low rates of vaccination; and
(4) include the dissemination of scientific and evidence-based vaccine-related information, such as-
(A) advancements in evidence-based research related to diseases that may be prevented by vaccines and vaccine development;
(B) information on vaccinations for individuals and communities, including individuals for whom vaccines are not recommended by the Advisory Committee for Immunization Practices, and the effects of low vaccination rates within a community on such individuals;
(C) information on diseases that may be prevented by vaccines; and
(D) information on vaccine safety and the systems in place to monitor vaccine safety.
The Public Readiness and Emergency Preparedness Act (PREPA), passed by the United States Congress and signed into law by President of the United StatesGeorge W. Bush in December 2005 (as part of Pub.L.109–148 (text)(PDF)), is a controversial tort liability shield intended to protect vaccine manufacturers from financial risk in the event of a declared public health emergency. The part of PREPA that actually affords such protection is now codified at 42 U.S.C.§ 247d-6d. The act specifically affords to drug makers immunity from actions related to the manufacture, testing, development, distribution, administration and use of medical countermeasures against chemical, biological, radiological and nuclear agents of terrorism, epidemics, and pandemics. PREPA strengthens and consolidates the oversight of litigation against pharmaceutical companies under the purview of the secretary of Health and Human Services (HHS). PREPA provides $3.8 billion for pandemicinfluenza preparedness to protect public health in the case of a pandemicdisease outbreak.
Vaccine manufacturers lobbied for the legislation, which would effectively preempt state vaccine safety laws in the case of an emergency declaration by HHS, by making clear they would not produce new vaccines unless the legislation was enacted.
During and in the aftermath of the 2020-21 COVID-19 pandemic in the United States, PREPA is being invoked in a variety of lawsuits, many involving skilled nursing or assisted living facilities where COVID-19 countermeasures including the administration or non-administration of vaccines is said to have resulted in or contributed to resident deaths.[1] Although PREPA was around for more than 15 years, prior to COVID-19, the act's defensive application in litigation was not widespread, but now the application of the act is being included more frequently in a variety of COVID-19 related lawsuits, including Shareholder Derivative Litigation.[2]
The Public Readiness and Emergency Preparedness Act (PREP Act) authorizes the Secretary of the Department of Health and Human Services (Secretary) to issue a PREP Act declaration. The declaration provides immunity from liability (except for willful misconduct) for claims:
of loss caused, arising out of, relating to, or resulting from administration or use of countermeasures to diseases, threats and conditions
determined by the Secretary to constitute a present, or credible risk of a future public health emergency
to entities and individuals involved in the development, manufacture, testing, distribution, administration, and use of such countermeasures
The negotiators agreed to exactly $10 billion in offsets by tapping unspent funds from prior pandemic aid laws. The measure would claw back the following unused appropriations:
$2.3 billion from a program intended to keep aviation manufacturing workers on payroll.
$1.9 billion each from unused grans for shuttered live entertainment venues and a state small business credit program.
$1.6 billion for Agriculture Department aid to commodity producers, food banks and others.
$900 million for the Small Business Administration's econoic injury disaster loan program.
$887 million from local and tribal assistance funds, with the addition of flexibility for state, localities and tribes to use existing funds for infrastucture-related spending, based on a Senate-passed bill from John Cornyn, R-Texas, and Alex Padilla, D-Calif.
$500 million from aid to colleges and universities.
"Importantly, this bill is comprised of dollar-for-dollar offsets and will not cost the American people a single additional dollar," Sen. Mitt Romney, R-Utah, one of the lead GOP negotiators, said in a statement announcing the deal.
The Justice Department has quietly asked Congress for the ability to ask chief judges to detain people indefinitely without trial during emergencies — part of a push for new powers that comes as the novel coronavirus spreads throughout the United States.
politico.com [2020-06-08] By BETSY WOODRUFF SWAN, 03/21/2020 link archive General
As a result of the continued consequences of the Coronavirus Disease 2019 (COVID-19) pandemic, on this date and after consultation with public health officials as necessary, I, Xavier Becerra, Secretary of Health and Human Services, pursuant to the authority vested in me under section 319 of the Public Health Service Act, do hereby renew, effective July 15, 2022, the January 31, 2020, determination by former Secretary Alex M. Azar II, that he previously renewed on April 21, 2020, July 23, 2020, October 2, 2020, and January 7, 2021, and that I renewed on April 15, 2021, July 19, 2021, October 15, 2021, January 14, 2022, and April 12, 2022, that a public health emergency exists and has existed since January 27, 2020, nationwide.
aspr.hhs.gov [2022-07-27] HHS, Administration for Strategic Preparedness and Response (ASPR), July 15, 2022 link archive General
The US HHS Administrative state has extended the COVID medical emergency. Let's look at the data.
Senator Rand Paul has accused Dr. Fauci and the White House (which is captured by the HHS Administrative State) of “emotionalism and sensationalism” leading up to the renewal of the determination of a continuing medical emergency attributable to COVID-19 disease and SARS-CoV-2 infection.
Is this medical emergency justified, or does it reflect yet more mis- dis- and mal-information from the HHS Administrative state acting in coordination with corporate media to propagate Fearporn to justify the continuing suspension of medical ethics, normal regulatory process, censorship, and war profiteering by the medical-pharmaceutical industrial complex?
“After White House adviser Dr. Anthony Fauci and Health and Human Services Secretary Xavier Becerra issued warnings about a new COVID-19 subvariant, Sen. Rand Paul (R-Ky.) said they are not providing key facts about the latest strain.
“How come the flu vaccine changes every year and they’re not willing to change this vaccine?” Paul told Fox News on Tuesday. “Now, you might have me with an argument. I’ll listen to you if you tell me, ‘We’ve got a new vaccine that actually has something to do with the current virus,'” he said.
It came after Fauci, who has given hundreds of media interviews since the start of the pandemic, told CNN this week that the Omicron subvariant BA.5 is concerning due to its high transmissibility. People infected in the first COVID-19 waves “really don’t have a lot of good protection” against the latest subvariant, Fauci also said at a White House briefing several days ago.
But Paul, himself a doctor, told Fox that Omicron “was about 90 percent less likely to put you in the hospital than the first variant,” saying that Americans should “discount” what both Fauci and Becerra are saying about the latest subvariant.
“So if no one’s telling you any information, how can you make any judgment other than the emotionalism and the sensationalism of the government?” he asked.”
Let’s look at the data using the slide format that so many seem to find useful. Minimal interpretation, mainly just data. I give you the tools, you make your own assessment and determination. What do you think is going on here?
The Biden administration on Thursday extended the nation’s COVID-19 public health emergency for the next 90 days as officials brace for a potential surge of infections over the winter.
The declaration comes as daily deaths and case rates have been falling, though the U.S. continues to see more than 300 people dying due to COVID-19 each day.
White House health officials have been urging people to get the updated variant-specific COVID-19 vaccine, and have said the extent of any surge depends on the precautions people take and the vaccination rates.
“If you are up to date with your vaccines and if you get treated, if you have a breakthrough infection, your risk of dying from COVID is now close to zero,” White House COVID-19 response coordinator Ashish Jha said Tuesday.
“We know there’s more work to do with real challenges ahead of us as we head into the fall and winter and the holidays. We’re doing everything we can as an administration to stay ahead of this virus. But if we all do our part — not just us in the administration, but Congress and the American people — I remain incredibly confident we can manage this virus for this fall and winter with less suffering and we can have a safe and healthy holiday season ahead,” Jha said.
The public health emergency was first declared in January 2020, and has been renewed every 90 days since.
[...]
See related data element: CDC ADDS COVID SHOT TO CHILDHOOD SCHEDULE
thehill.com [2022-10-20] NATHANIEL WEIXEL, 10/13/22 link archive General
As a result of the continued consequences of the Coronavirus Disease 2019 (COVID-19) pandemic, on this date and after consultation with public health officials as necessary, I, Xavier Becerra, Secretary of Health and Human Services, pursuant to the authority vested in me under section 319 of the Public Health Service Act, do hereby renew, effective October 13, 2022, the January 31, 2020, determination by former Secretary Alex M. Azar II, that he previously renewed on April 21, 2020, July 23, 2020, October 2, 2020, and January 7, 2021, and that I renewed on April 15, 2021, July 19, 2021, October 15, 2021, January 14, 2022, April 12, 2022, and July 15, 2022, that a public health emergency exists and has existed since January 27, 2020, nationwide.
October 13, 2022 _____________________________ Date
/s/ _____________________________ Xavier Becerra
aspr.hhs.gov [2022-10-25] Xavier Becerra, October 13, 2022 link archive General
Stop the Abuses of Power, Corruption, and Fiscal Irresponsibility
The National COVID-19 Emergency, first declared by President Trump in March 2020 in response to the COVID-19 pandemic, was formally extended a second time by President Biden on February 18, 2022 and will come up for a third consideration by Biden in February, 2023. In January 2020, the U.S. Department of Health and Human Services (HHS) declared a public health emergency (PHE) in response to the outbreak of COVID-19. Public health emergency declarations ease certain laws and regulations to make it easier to address the emergency and allow some federal grant money to flow toward addressing the emergency. A PHE is a lesser event than a national emergency, which triggers a rapid outlay of federal money to address the emergency. National emergencies also give great unliteral power to the president, allowing the president to do things such direct flows of money from the national treasury, deploy the national guard, etc.
From a clinical point of view from a physician who has treated COVID-19 from the very beginning, a PHE would be evident if hospital capacity was exceeded by COVID-19 patients and care could not be provided to other patients with urgent problems. As a general rule this would be >15% occupancy by COVID-19 patients. From that perspective, the COVID-19 PHE ended in January, 2021 once hospital capacity ramped up to meet demand. I checked the CDC website and the weekly cases of COVID-19 has maintained its unimpressive pattern of oscillations while hospitalized cases are about 5000 well below that 15% threshold of about 130,0000.
[...]
In summary, both national emergencies and PHE are power grabs that facilitate unchecked decisions and flows of money fostering corruption and continued desire to extend the declarations. The House and the Senate figured this out back in the 1970’s and found a legislative way of ending them. Until these declarations are dropped, we will continue to careen out of control on health policy, pandemic response, corruption, and fiscal irresponsibility. The most important question you can can ask a lawmaker, governor, or president or candidate: “Are you in favor of dropping the emergency declaration and PHE? If not why?
What does the "intent to end" on May 11, 2023 actually mean for you?
Finally, we may be seeing a winding down of US Federal Government responses to the COVIDcrisis. January 30, 2023 is a date destined to go down in history as the beginning of the end of the draconian US Federal Government’s “public health” measures, which have been implemented in a step wise (ratcheting) manner beginning late January, 2020. What does this really mean, in a practical, real-world, kitchen-table sense of things?
Depending on when you define the point in time where SARS-CoV-2 entered the population of humans, the COVIDcrisis has extended for about three years- in contrast to the two year long “1918 Swine Flu” epidemic involving a different RNA respiratory virus attributed to causing over 50 million deaths world wide. As of January 31, 2023, there have been 6,812,798 cumulative deaths from COVID-19 per the WHO.
[...]
rwmalonemd.substack.com [2023-02-07] Robert W Malone MD, MS, February 6, 2023 link archive General
The Covid emergency is over in America…in three more months says the White House. Why now? Is politics at the heart of this decision? And what does it mean for the EUA vaccines and therapies? The HighWire gets to the facts behind the headlines.
HHS Secretary Xavier Becerra sent a letter to U.S. governors with the surprise announcement. Becerra wrote:
"Based on current trends regarding COVID-19, the U.S. Department of Health and Human Services is planning for this to be the final renewal and for the COVID-19 PHE to end on May 11, 2023."
and
"Rather than 60 days' notice, I am providing 90 days' notice before the COVID-19 PHE ends to give you and your communities ample time to transition."
HHS appended a “fact sheet” to the letter with information on exactly what administrative and regulatory policies and rules will and will not be affected.
On February 9, 2023, the Secretary of Health and Human Services (HHS) renewed the Coronavirus Disease 2019 (COVID-19) public health emergency declaration issued under section 319 of the Public Health Service Act (PHS Act) (“PHE declaration”), effective February 11, 2023. The declaration is expected to expire at the end of the day on May 11, 2023. The Food and Drug Administration (FDA, Agency, or we) has issued guidance documents to address the circumstances of the public health emergency and, more generally, COVID-19. Many of those guidance documents are tied to the duration of the PHE declaration. This notice is intended to provide clarity to stakeholders with respect to the guidance documents that will no longer be effective with the expiration of the PHE declaration and the guidances that FDA is revising to continue in effect after the expiration of the PHE declaration.
Long-term Underinvestment in Public Health Infrastructure and Longstanding Health Disparities Put the Nation at Increased Risk from the Coronavirus.
Before the Coronavirus Crisis, the United States Had Not Sufficiently Invested in Pandemic Preparedness, Despite Well-Known Risks.
The Trump Administration’s Failed Stewardship Over the Pandemic Response and Persistent Pattern of Political Interference Undermined the Nation’s Ability to Respond to the Pandemic.
The Toll of the Coronavirus Fell Disproportionately on the Most Vulnerable.
Life-Saving Vaccinations and the Biden Administration’s Stewardship Helped the Nation Emerge from the Coronavirus Crisis, Yet Decisions Made by the Trump Administration, Actions Taken by Private Companies, and Predatory Actors Spreading Misinformation Have Undermined These Efforts.
[...]
As the Coronavirus Crisis Upended the U.S. Economy, Longstanding Inadequate Protections for Workers Put America’s Families at Increased Risk.
Congress Passed Rapid, Aggressive Federal Relief to Save Lives and Reduce Economic Damage, Which Compensated for Structural Weaknesses.
The Trump Administration Failed to Prioritize and Effectively Deliver Relief for Working Americans.
Poor Implementation and Oversight of Federal Aid Programs, Combined with Unscrupulous Private Actors, Led to Significant Waste, Fraud, and Abuse and a Less Effective Pandemic Response.
Congress and the Biden Administration Improved the Federal Implementation of Pandemic Programs, Addressed Earlier Failures, and Supported a Robust and Equitable Jobs Recovery.
House Select Subcommittee on the Corona Crisis' Final Report is a disaster
[...]
* Finally, buried at #8, we find the verbiage that will allow Congress to give the WHO sovereignty under the guise of a public health response: Recommendation: The federal government should increase its collaboration with international partners to strengthen its ability to protect people from future threats and mount a coordinated, effective, and equitable response to major global health crises when they do occur.
coronavirus.house.gov [2022-12-18] (pdf doc) SELECT SUBCOMMITTEE on the CORONAVIRUS CRISIS, DECEMBER 2022 link archive General
Tuesday, House Select Subcommittee on the Coronavirus Pandemic Chairman Brad Wenstrup from Ohio held a roundtable discussion titled “Preparing For the Future By Learning From the Past: Examining COVID Policy Decisions”. The goal of this roundtable, as stated on the House Oversight website, was to “discuss COVID-19 policy decisions with renowned doctors to thoroughly examine the federal government’s response to the COVID-19 pandemic.”
[...]
The Roundtable
The recently formed, bi-partisan COVID subcommittee kicked off its first roundtable discussion yesterday. There were witnesses brought by both Democrats and Republicans to answer questions and speak about their experiences through COVID.
The Panel:
Dr. Martin Kulldorff is an epidemiologist and biostatistician, as well as a Professor of Medicine (on leave) at Harvard. He is an original co-author of The Great Barrington Declaration, which advocated for focused protection as a strategy against COVID, instead of lockdowns in 2020.
Dr. Marty Makary is the Chief of Islet Transplant Surgery at Johns Hopkins, as well as a public health researcher and healthcare expert at John Hopkins University. Dr. Makary has over 250 peer-reviewed scientific articles and has been elected to the National Academy of Medicine.
Dr. Jay Battacharya is a Professor at Stanford School of Medicine. He’s been a champion for Medical Freedom since early on in the pandemic, and he was one of the first people to be censored on Twitter for his COVID views.
Dr. Georges Benjamin, the executive director of the American Public Health Association represented a defense of the government’s COVID response.
Dr. Martin Kulldorfstarted off with a strong statement: “During the last few years, we have seen the worst public health mistakes in history”
Dr. Jay Battacharya addressed the widespread harms that occurred due to lockdowns, and the high number of COVID deaths even with harsh measures that trampled on civil liberties. “At best, they [lockdowns] temporarily protected the Laptop Class who could work from home without losing their jobs, about 30% of the population, while being served by the working class.”
Dr. Makary brought several crucial bits of information to light: He condemned the notion of injecting children. “Has any young, healthy child died in the United States of COVID? In the last three years?” he asked. “Germany did a study — it was zero kids, 5 through 11 years of age, that died that were healthy in that entire country.”
Dr. Makary mentioned the government’s decision to not recognize natural immunity. And to no one’s shock, Fauci played a big role in that decision. “He just decided … that if you have circulating antibodies that neutralize the virus, they’re antibodies the government does not recognize unless they were derived from the vaccine.”
WASHINGTON, D.C. – The House Judiciary Subcommittee on the Constitution and Limited Government will hold a hearing on Tuesday, April 16, 2024, at 2:00 p.m. ET. The hearing, "Liberty, Tyranny, and Accountability: Covid-19 and the Constitution," will examine the federal and state responses to the Covid-19 pandemic and the effects on the civil liberties of Americans.
WITNESSES:
Harmeet Dhillon, Founder and CEO, Center for American Liberty
Dr. Joseph Ladapo, State Surgeon General of Florida
Beanie Geoghegan, Co-Founder, Freedom in Education
One doctor in Austin literally got a taste of his own medicine after going to his own practice to get a Covid antibody test. Assuming he would get one for free because he worked for the company, his insurance instead wound up getting a bill from Physicians Premier ER for $10,984. His insurance paid it all.
truepundit.com [2020-09-12] September 11, 2020 link archive General
Congress has approved some $4.5 trillion in total aid spending. Federal agencies have formally committed to using about $4 trillion of that, and have made $3.5 trillion in actual payments to date.
It can often take time for the total pot of funds approved by lawmakers to make its way to the American people, budget experts say.
Education, health care and disaster relief are among the areas where the government has underspent the funds, according to a CNBC analysis.
[...]
cnbc.com [2022-11-26] Nate Rattner, Jacob Pramuk, DEC 9 2021 link archive General
Historically (as was the case in World War II) a crisis typically arose in the form of an aggressive foreign power. James Madison observed that the trouble with an established military interest is that, because it accrues its wealth, power, glory, and prestige from waging war, it is necessarily interested in waging wars instead of averting them.
The same can now be said of emerging infectious diseases. Instead of armed soldiers threatening us, we are menaced by invisible pathogens. Instead of Lockheed Martin and Raytheon receiving the federal money gravy train, it’s Pfizer, Moderna, and the rest of the Bio-Pharmaceutical Complex that has been positioning itself for the next (“certain to emerge”) infectious disease.
The legal framework for this bonanza was established by the PREP Act (Public Readiness and Emergency Preparedness) of 2005. This authorized the Secretary of Health and Human Services to deploy a wide array of “Emergency Countermeasures” in the event of an infectious disease outbreak. When invoked by the HHS Secretary, the PREP Act provides immunity for the “manufacture, testing, development, distribution, administration, and use of covered countermeasures.” On February 4, 2020, HHS Secretary Alex Azar declared COVID-19 an emergency and invoked the PREP Act.
Pursuant to the PREP Act, the CARES Act of March 27, 2020—passed within the context of a “public health emergency”—created $2 trillion with the stroke of a keyboard. These funds were disbursed to a host of companies, individuals, and institutions in the business of infectious disease “countermeasures.” The Act was reminiscent of the Emergency Economic Stabilization Act of 2008 for bailing out Wall Street.
Because the mRNA vaccines fall under the PREP Act definition of “emergency countermeasures,” their production is not subjected to the same testing and quality control regulations as licensed pharmaceutical products. Their production and deployment resemble that of military products during World War II. For example, many aircraft hastily designed and manufactured for that cataclysm were so dangerous and unreliable that far more servicemen were killed in training and routine flight accidents than in combat. The fabled Vought F4U Corsair was known as the “Ensign Eliminator” because its dreadful stall characteristics killed so many young airman.
[...]
petermcculloughmd.substack.com [2022-12-10] John Leake, December 9, 2022 link archive General
Since the start of the coronavirus pandemic, Congress, states, and both the Trump and Biden Administrations have adopted a number of policies to ease financial pressure on hospitals and other health care providers. The infusion of funds was intended to help alleviate the fiscal impact of revenue loss due to delays in non-urgent care, coupled with new costs associated with COVID-19. With the recent increase in Omicron-related cases, hospitalizations and deaths, this brief describes the main sources of federal funds for health care providers and how those funds have been allocated. It also describes federal spending for COVID-19 testing, including at-home testing, using the most recent data available (as of September 2021).
Federal Funding for Hospitals and Other Health Care Providers During the Pandemic: Key Sources of Federal Support
Congress established the Provider Relief Fund to bolster hospitals and other health care providers to compensate for financial losses and unanticipated costs during the pandemic. HHS has allocated $170.9 billion of the total $178 billion authorized by Congress for this Fund as of September 2021, including $14.8 billion used to support vaccine development and distribution. Of the total amount, $143 billion has been disbursed, according to GAO and HHS announcements. HHS expects to distribute another $6 billion to providers in early 2022.
In addition, $7.5 billion of $8.5 billion in American Rescue Plan (ARP) rural funds were distributed to hospitals and other providers that serve patients living in rural areas; the remaining $1 billion in rural funds is expected to be distributed in early 2022.
Congress took several steps to avoid automatic payment reductions during the pandemic. Congress waived the automatic 2% reduction in Medicare payments required under budget rules (i.e., sequestration) between May 1, 2020 and March 31, 2022, delayed until 2023 a separate 4% reduction in Medicare payments that would otherwise have been triggered in 2022 under PAYGO rules, and increased physician payments by 3% for 2022 under the Medicare Physician Fee Schedule (PFS) payments to mitigate scheduled budget neutral cuts.
Congress established the Paycheck Protection Program that provided health care providers an estimated $100 billion in Paycheck Protection Program (PPP) loans, according to MedPAC.
In addition, Congress increased Medicare payments for inpatient COVID-19 admissions by 20% during the public health emergency (PHE), established coverage and payment for administering COVID-19 vaccines, and increased payments for telehealth services, and HHS waived certain regulatory restrictions, such as allowing for expanded coverage of Medicare telehealth services. Congress also provided accelerated or advance payments as loans to providers participating in traditional Medicare to ease cash flow disruptions during the pandemic.
[...]
Reimbursement for COVID-19 vaccination administration: Medicare increased its reimbursement for COVID-19 vaccine administration from $17 for an initial dose in a series and $28 for the final dose in a series to approximately $40 per dose. This also applies to booster doses approved by the FDA under the emergency use authorizations. As of June 2021, Medicare also pays an additional $35 per dose for administering the COVID-19 vaccine in the home for certain Medicare patients. Most states have policies in place to increase Medicaid payments for COVID-19 vaccine administration to 100% of the Medicare rate. Medicare and Medicaid beneficiaries are not subject to any cost sharing for the COVID-19 vaccine and administration. For the uninsured and underinsured, a portion of the Provider Relief Funds are being used to reimburse providers for administering COVID-19 vaccines to uninsured or underinsured individuals.
[...]
kff.org [2023-04-11] Nancy Ochieng, Jeannie Fuglesten Biniek, MaryBeth Musumeci, Tricia Neuman, Jan 27, 2022 link archive General
The claim: Hospitals get paid more if patients are listed as COVID-19, and on ventilators
Sen. Scott Jensen, R-Minn., a physician in Minnesota, was interviewed by "The Ingraham Angle" host Laura Ingraham on April 8 on Fox News and claimed hospitals get paid more if Medicare patients are listed as having COVID-19 and get three times as much money if they need a ventilator.
"How can anyone not believe that increasing the number of COVID-19 deaths may create an avenue for states to receive a larger portion of federal dollars. Already some states are complaining that they are not getting enough of the CARES Act dollars because they are having significantly more proportional COVID-19 deaths."
[...]
Our ruling: True
We rate the claim that hospitals get paid more if patients are listed as COVID-19 and on ventilators as TRUE.
Hospitals and doctors do get paid more for Medicare patients diagnosed with COVID-19 or if it's considered presumed they have COVID-19 absent a laboratory-confirmed test, and three times more if the patients are placed on a ventilator to cover the cost of care and loss of business resulting from a shift in focus to treat COVID-19 cases.
[...]
usatoday.com [2023-05-06] Michelle Rogers, April 24, 2020 link archive General
Untold numbers of Americans have gone without medical care for more than a year now, resulting in health conditions becoming worse, diagnoses being missed, unmeasurable stress for anxious patients and families, and worsening prognoses.
One reason people haven't received care has been ignored in the media, but reveals a disturbing decline of ethics in medicine and politics: The healthcare industry has been using Covid-19 screening tests to deny care to patients who do not want the test.
remnantnewspaper.com [2021-03-12] by Sandy Szwarc, March 6, 2021 link archive General
As exposed in audio recordings, hospital executives in Arizona admitted meeting several times a week to lower standards of care, with coordinated restrictions on visitation rights. Most COVID-19 patients’ families are deliberately kept in the dark about what is really being done to their loved ones.
The combination that enables this tragic and avoidable loss of hundreds of thousands of lives includes (1) The CARES Act, which provides hospitals with bonus incentive payments for all things related to COVID-19 (testing, diagnosing, admitting to hospital, use of remdesivir and ventilators, reporting COVID-19 deaths, and vaccinations) and (2) waivers of customary and long-standing patient rights by the Centers for Medicare and Medicaid Services (CMS).
[...]
Creating a “National Pandemic Emergency” provided justification for such sweeping actions that override individual physician medical decision-making and patients’ rights. The CARES Act provides incentives for hospitals to use treatments dictated solely by the federal government under the auspices of the NIH. These “bounties” must paid back if not “earned” by making the COVID-19 diagnosis and following the COVID-19 protocol.
The hospital payments include:
A “free” required PCR test in the Emergency Room or upon admission for every patient, with government-paid fee to hospital.
Added bonus payment for each positive COVID-19 diagnosis.
Another bonus for a COVID-19 admission to the hospital.
A 20 percent “boost” bonus payment from Medicare on the entire hospital bill for use of remdesivir instead of medicines such as Ivermectin.
Another and larger bonus payment to the hospital if a COVID-19 patient is mechanically ventilated.
More money to the hospital if cause of death is listed as COVID-19, even if patient did not die directly of COVID-19.
A COVID-19 diagnosis also provides extra payments to coroners.
[...]
citizensjournal.us [2022-03-03] Elizabeth Lee Vliet, Ali Shultz, DECEMBER 21, 2021 link archive General
On Thursday, March 11, 2021, the American Rescue Plan (ARP) Act was signed into law. It is an unprecedented $1.9 trillion package of assistance measures, including $122 billion for the ARP Elementary and Secondary School Emergency Relief (ARP ESSER) Fund. Funds are provided to State educational agencies and school districts to help safely reopen and sustain the safe operation of schools and address the impact of the coronavirus pandemic on the Nation’s students.
The ARP ESSER Fact Sheet, published on March 17, 2021, provides an overview of the program and a comparison of the ESSER Fund (funded through the CARES Act), ESSER II Fund (funded through the CRRSA Act), and ARP ESSER Fund (ARP Act).
[...] Tennessee is receiving more than $2 billion total in ARP ESSER funds, and today's approval of their plan will result in the release of the final $830 million. [...]
HHS recently began distributing the first $30 billion of emergency funding designated for hospitals in the Coronavirus Aid, Relief, and Economic Security Act. Some of the states hit hardest by the COVID-19 pandemic will receive less funding than states touched relatively lightly, according to an analysis by Kaiser Health News.
The first round of grants will be distributed based on historical share Medicare revenue, not based on COVID-19 burden. Therefore, hard-hit states like New York will receive far less per COVID-19 case than most other states.
HHS said it doled out the first slice of funding based on Medicare revenue to get support to hospitals as quickly as possible. The agency said the next round of grants "will focus on providers in areas particularly impacted by the COVID-19 outbreak," rural hospitals and other healthcare providers that receive much of their revenues from Medicaid.
Below is a breakdown of how much funding per COVID-19 case each state will receive from the first $30 billion in aid. Kaiser Health News used a state breakdown provided to the House Ways and Means Committee by HHS along with COVID-19 cases tabulated by The New York Times for its analysis.
[... state by state listing follows ...]
beckershospitalreview.com [2022-01-11] Ayla Ellison, April 14, 2020 link archive General
We know hospitals are getting marching orders from the American Hospital Association (AHA) and our state health department. Here is a special bulletin from AHA regarding these funds. This special bulletin from AHA describes eligibility and distribution of funds.
Tennessee hospitals receive even more money for every COVID case based on COVID relief legislation that created a 20 percent premium (or "add on") for Medicare patients. (Source: USA Today, Fox News, Healthcare Compliance Association)
Our Governor, Bill Lee, and the Financial Stimulus Accountability Group (FSAG) released recommendations in early October 2021 for additional investment of federal relief dollars ($3 billion), so there is currently no end to the medical murder for money scheme. (Source: SpartaLive.com)
[...]
theadamgroup.net [2022-01-11] The Adam Group link archive General
Congress set up a massive, $178 billion fund in 2020 meant to help mitigate the impacts of the Covid-19 pandemic on health care providers, known as the Provider Relief Fund.
The Trump and Biden administrations haven’t always been reliable about sending out the money — or sending it on time. But STAT’s new analysis of a Health and Human Services database of the money reveals where it’s flowing and who has received the most so far.
By far, the largest payments were made to the nation’s biggest hospital systems. Fully five of the top 10 recipients of cash were New York City-area hospitals or health systems; together, they received some $3.1 billion. The New York and Presbyterian Hospital (usually styled “NewYork-Presbyterian”) alone brought in $631 million, topped only by the $1.2 billion that went to the New York City Health and Hospitals Corporation, a group that operates New York City’s sprawling system of public hospitals and clinics.
STAT is publishing the entire database here in a searchable and sortable format.
Many smaller providers also benefited from the program. Of the 412,591 payments published so far, the median was just $12,530. Ninety percent of all payments were below $192,569.
[...]
statnews.com [2022-04-02] By J. Emory Parker, Sept. 24, 2021 link archive General
April 08, 2020 - Hospital reimbursement for the treatment of uninsured COVID-19 patients could account for more than 40 percent of the $100 billion earmarked for hospitals in the latest coronavirus stimulus package, according to estimates from the Kaiser Family Foundation.
In a new issue brief, researchers from the Kaiser Family Foundation estimated total hospital reimbursement to range from $13.9 billion to $41.8 billion depending on the rate of and severity of COVID-19 hospitalizations among the uninsured population.
That reimbursement range is based on Medicare reimbursement for hospitals admissions for similar conditions, including respiratory infections and inflammations with major comorbidities or complications, which averaged $13,297 in reimbursements, and, in more severe cases, respiratory system diagnosis with ventilator support for greater than 96 hours, which averaged $40,218.
Researchers also estimated that up to 2 million uninsured individuals could require hospitalization for COVID-19. Although, that number could be as low as 670,000 hospitalizations.
[...]
revcycleintelligence.com [2022-02-04] By Jacqueline LaPointe, April 08, 2020 link archive General
CMS issued an Interim Final Rule with Comment Period that established the New COVID-19 Treatments Add-on Payment (NCTAP) under the Medicare Inpatient Prospective Payment System (IPPS). The NCTAP, designed to mitigate potential financial disincentives for hospitals to provide new COVID-19 treatments, is effective from November 2, 2020, until the end of the COVID-19 public health emergency (PHE).
Through the NCTAP, the Medicare Program will provide an enhanced payment for eligible inpatient cases that use certain new products with current FDA approval or emergency use authorization (EUA) to treat COVID-19, including the following:
On August 23, 2020, the FDA issued (reissued on November 30, 2020, and revised on March 9, 2021) an EUA for the use of COVID-19 convalescent plasma for treating COVID-19 in hospitalized patients
On October 22, 2020, the FDA approved remdesivir (Veklury) for the treatment of COVID-19 for adults and certain pediatric patients requiring hospitalization
On November 19, 2020, the FDA issued (and amended on December 20, 2021) an EUA for the use of baricitinib (Olumiant) for the treatment of suspected or laboratory confirmed COVID-19 in certain hospitalized patients
On December 22, 2021, the FDA issued an EUA for molnupiravir for the treatment of mild-to-moderate COVID-19 in certain adults who are at high-risk for progression to severe COVID-19, including hospitalization or death.
On December 23, 2021, the FDA issued an EUA for nirmatrelvir (Paxlovid) for the treatment of mild-to-moderate COVID-19 in certain adults and pediatric patients at high risk for progression to severe COVID-19, including hospitalization or death.
For eligible cases, the NCTAP is equal to the lesser of these:
65% of the operating outlier threshold for the claim
NCTAP claims are those that are eligible for the 20% add-on payment under Section 3710 of the CARES Act. Eligible claims have an ICD-10-CM diagnosis code U07.1 (COVID-19) and one of the following:
ICD-10-PCS codes for remdesivir (Veklury), COVID-19 convalescent plasma, or baricitinib (Olumiant).
National Drug Codes (NDC) for nirmatrelvir and molnupiravir
Codes for Remdesivir or COVID-19 Convalescent Plasma for Hospital Discharges on or after November 2, 2020
Upon admission to a once-trusted hospital, American patients with COVID-19 become virtual prisoners, subjected to a rigid treatment protocol with roots in Ezekiel Emanuel’s “Complete Lives System” for rationing medical care in those over age 50. They have a shockingly high mortality rate. How and why is this happening, and what can be done about it?
As exposed in audio recordings, hospital executives in Arizona admitted meeting several times a week to lower standards of care, with coordinated restrictions on visitation rights. Most COVID-19 patients’ families are deliberately kept in the dark about what is really being done to their loved ones.
The combination that enables this tragic and avoidable loss of hundreds of thousands of lives includes (1) The CARES Act, which provides hospitals with bonus incentive payments for all things related to COVID-19 (testing, diagnosing, admitting to hospital, use of remdesivir and ventilators, reporting COVID-19 deaths, and vaccinations) and (2) waivers of customary and long-standing patient rights by the Centers for Medicare and Medicaid Services (CMS).
In 2020, the Texas Hospital Association submitted requests for waivers to CMS. According to Texas attorney Jerri Ward, “CMS has granted ‘waivers’ of federal law regarding patient rights. Specifically, CMS purports to allow hospitals to violate the rights of patients or their surrogates with regard to medical record access, to have patient visitation, and to be free from seclusion.” She notes that “rights do not come from the hospital or CMS and cannot be waived, as that is the antithesis of a ‘right.’ The purported waivers are meant to isolate and gain total control over the patient and to deny patient and patient’s decision-maker the ability to exercise informed consent.”
Creating a “National Pandemic Emergency” provided justification for such sweeping actions that override individual physician medical decision-making and patients’ rights. The CARES Act provides incentives for hospitals to use treatments dictated solely by the federal government under the auspices of the NIH. These “bounties” must be paid back if not “earned” by making the COVID-19 diagnosis and following the COVID-19 protocol.
The hospital payments include:
A “free” required PCR test in the Emergency Room or upon admission for every patient, with government-paid fee to hospital.
Added bonus payment for each positive COVID-19 diagnosis.
Another bonus for a COVID-19 admission to the hospital.
A 20 percent “boost” bonus payment from Medicare on the entire hospital bill for use of remdesivir instead of medicines such as Ivermectin.
Another and larger bonus payment to the hospital if a COVID-19 patient is mechanically ventilated.
More money to the hospital if cause of death is listed as COVID-19, even if patient did not die directly of COVID-19.
A COVID-19 diagnosis also provides extra payments to coroners.
CMS implemented “value-based” payment programs that track data such as how many workers at a healthcare facility receive a COVID-19 vaccine. Now we see why many hospitals implemented COVID-19 vaccine mandates. They are paid more.
[...]
stevenyager.org [2023-04-17] Steve Yager, Elizabeth Lee Vliet, Ali Shultz, Jan 23, 2022 link archive General
As reported last week by The Defender, federal monies from the 2020 and 2021 COVID stimulus bills dramatically reshaped K-12 educational priorities, turning American school officials into lackeys for federal agencies more intent on masking and vaccinating every last child than on supporting meaningful education.
So, too, with the stimulus-induced reshaping of hospital priorities.
In the second half of a January interview on Del Bigtree’s “The Highwire” — “COVID-19: Following the Money” — policy analyst A.J. DePriest reported on the untoward consequences set into motion as a result of COVID funds provided to hospitals.
Managed by the U.S. Department of Health and Human Services (HHS), the federal government allocated a total of $186.5 billion to the Provider Relief Fund (PRF), with two-thirds ($121.3 billion) disbursed as of January 2022.
The first tranche of $50 billion for hospitals and other Medicare providers — “for healthcare-related expenses or lost revenues … attributable to COVID-19” — began flying out the door in April 2020.
Almost immediately, alert doctors and astute journalists warned the Medicare add-on payments built into the relief package created perverse incentives unfriendly to patients’ interests.
As summarized by Dr. Scott Jensen — former Minnesota state senator and current gubernatorial candidate — “anytime healthcare intersects with dollars it gets awkward.”
Nearly two years down the road, the “awkwardness” is increasingly difficult to hide.
In the view of DePriest and many others, HHS’s stimulus slush fund has been every bit as dangerous for hospital patients as the U.S. Department of Education’s handouts have been for the nation’s schoolchildren.
Making out like bandits
Dr. Elizabeth Lee Vliet and Ali Shultz, J.D., who wrote a widely distributed op-ed in late 2021 for the Association of American Physicians and Surgeons (AAPS), summed up the disturbing situation prevailing in hospitals. The AAPS’s professional calling card is its “dedication to the highest ethical standards of the Oath of Hippocrates.”
Not mincing their words, the two argued that Centers for Medicare and Medicaid Services (CMS) payment directives turned hospitals and medical staff into “bounty hunters,” and COVID patients into “virtual prisoners.”
Highlighting the slew of CMS add-ons and other incentives established with the Coronavirus Aid, Relief and Economic Security (CARES) Act — and also the Paycheck Protection Program and Health Care Enhancement Act (PPPHCEA) — they emphasized the payments hinge on hospitals’ willingness to slavishly follow the National Institutes of Health’s (NIH’s) guidelines “for all things related to COVID-19.”
As itemized by Vliet and Shultz, compliant hospitals garner CMS payments for:
Each completed diagnostic test (required in the emergency room or upon admission).
Each COVID-19 diagnosis.
Each COVID admission.
Use of the intravenously administered Gilead drug remdesivir (brand name Veklury), which yields a 20% bonus payment on the entire hospital bill.
Mechanical ventilation.
COVID-19 listed as cause of death.
Citing a Becker’s Hospital Review breakdown, published in April 2020, of CARES Act payments to different states, DePriest told Bigtree payments ranged from $166,000 per COVID patient in Tennessee hospitals, for example, to far higher payments in states such as North Dakota ($339,000), Nebraska ($379,000) and West Virginia ($471,000).
In addition, for hospitals ascertained to be in COVID “hotspots,” HHS distributed special “high-impact” funds — $77,000 per admission initially, later downsized to $50,000 per admission.
HHS explained it used COVID admissions “as a proxy for the extent to which each facility experienced lost revenue and increased expenses associated with directly treating a substantial number of COVID-19 inpatient admission [sic].
[...]
childrenshealthdefense.org [2023-07-26] Children's Health Defense Team, January 24, 2022 link archive General
The claim: Blue Cross Blue Shield pays doctors bonuses based on the number of patients vaccinated
In an attempt to cast doubt on the safety and efficacy of COVID-19 vaccines, some online users are claiming pediatricians are paid a bonus by Blue Cross Blue Shield based on the percentage of patients they vaccinate.
“Blue Cross Blue Shield pays your doctor a $40,000 bonus for fully vaccinating 100 patients under the age of 2,” reads a Dec. 12, 2021, Instagram post that was shared by actress Cherie Johnson and accumulated more than 600 likes. “If your doctor manages to fully vaccinate 200 patients, that bonus jumps to $80,000.”
The post claims pediatricians lose the entire bonus unless at least 63% of patients are fully vaccinated, including the flu vaccine. It asserts, "This is why your doctor gets aggressive."
But Blue Cross Blue Shield doesn't provide incentives solely based on the number of patients vaccinated, as the post suggests. Incentive programs vary by state and require doctors to meet goals related to a number of different practices and services.
Bonuses not based solely on vaccines
Blue Cross and Blue Shield is a national federation of 35 independent and locally operated companies, each of which sets its own value-based contracts with local providers, according to an agency spokesperson.
“The purpose of any performance-based incentives, where they exist, is to reward implementation of well-established, evidence-based best practices in the care of our members,” a Blue Cross Blue Shield spokesperson said in an emailed statement. “While vaccinations may fall into that category, they would not be the sole performance measure.”
[...]
Our rating: Missing context
[...]
usatoday.com [2023-04-17] McKenzie Sadeghi, February 18, 2022 link archive General
But the riches get even richer for physicians during COVID-19!
A second incentive program was based on a bonus system for percent of patients vaccinated during the 2021 year. That document is as follows:
With an average patient to primary care physician ratio of 1800, lets do the numbers for the 2021 final incentive program for the seven month period (.58% of 12 months) beginning on January 1, 2021. Note: these are examples, based on 1800 a patient practice per physician.
30% of anthem members vaccinated within a practice x $20 (x .58) = $10,800.00
40% of anthem members vaccinated within a practice x $45 = $32,400.00
50% of anthem members vaccinated within a practice x $70 = $63,000.00
60% of anthem members vaccinated within a practice x $100 = $108,000.00
75% of anthem members vaccinated within a practice x $125 = $168,750.00
With a patient to primary care physician ratio of 1800, lets do the numbers for the 2021 final incentive program (which would have included children 12 and up) for the FIVE month period (.41% of 12 months) at the end of 2021.
30% of anthem members vaccinated within a practice x $100 (x .41) = $22,140
40% of anthem members vaccinated within a practice x $150 = $44,280.00
50% of anthem members vaccinated within a practice x $175 = $64,575.00
60% of anthem members vaccinated within a practice x $200 = $88,560.00
75% of anthem members vaccinated within a practice x $250 = $138,375.00
It appears that during 2021, the individual bonus plan and the percent vaccinated “incentive” program ran simultaneously.
If a practice managed to achieve a 75% vaccination rate, the bonus and incentive program would have yielded an extra profit somewhere in the range of $382,125.00 for 2021!
My example calculations (each practice numbers would vary):
You might recall that back in the very early days of Covid-19 (or just “coronavirus” as it was then known), some crypto nutters enthusiasts started getting excited about the idea that the virus would be good for bitcoin because “paper money” “might be the source of #CORONAVIRUS #SARS2 infection”. After all, “fiat is dirty”:
[...]
Now, to be fair to the bitcoin bros (not great) and XRP army (worse), even the World Health Organisation had around that time started pushing the idea that Covid could be being spread by banknotes (while simultaneously recommending that people should not wear masks), now thought to be “very unlikely”. Even if banknotes were a key transmission vector, however, we are not sure that “dirty fiat” itself could be held responsible, given that the vast majority of it only exists in digital form. Why would you use bitcoin, or XRP, or any other crypto token when you can transact digitally using fiat currencies? Yet in some ways, the crypto crowd were not wrong. In the almost 18 months since Covid-19 was declared a pandemic, the price of bitcoin has risen by about 525 per cent, from just under $8,000 to a three-month high just above $50,000 on Monday. XRP has climbed by a similar amount to trade around the $1.25 mark.
[...]
ft.com [2022-02-27] Jemima Kelly, AUGUST 24 2021 link archive General
“COVID fraud” is at this point a redundant phrase. Congress appropriated more than $5 trillion for COVID relief but almost $600 billion may have been lost to fraud — an astounding 12%. Washington’s pandemic pratfalls are the greatest federal boondoggle of this century.
Prosecutors are having a turkey shoot nailing COVID crooks: More than 1,500 have been indicted and almost 500 have been convicted. On September 14, the Justice Department announced the creation of three COVID-19 fraud strike force teams.
When President Biden recently signed a law to extend the time to prosecute COVID fraud, he declared, “My message to those cheats out there is this: You can’t hide. We’re going to find you.” But the sheer amount of fraud makes it unlikely that the vast majority of thieves will be charged.
Policymakers acted as if waiving standard federal fraud protections would somehow thwart the COVID virus. On September 22, the Labor Department inspector general estimated that COVID-19 unemployment fraud amounted to $45 billion and could exceed $163 billion. “Overseas organized crime groups flooded state unemployment systems with bogus online claims, overwhelming antiquated computer software benefits in blunt-force attacks that siphoned out millions of dollars,” NBC News reported.
Prison inmates, drug gangs and Nigerian racketeers easily plundered the program. One swindler collected unemployment benefits from 29 different states. In the first year of the pandemic, Maryland detected more than 1.3 million fraudulent unemployment claims — equal to 20% of the state’s population.
Beginning in June 2020, the feds distributed $813 billion in Paycheck Protection Program loans to businesses. President Donald Trump’s Treasury Secretary Steven Mnuchin boasted that PPP is “supporting an estimated 50 million jobs.” But many of those jobs existed solely in the imagination of political appointees.
The Small Business Administration (SBA), which administered the program, effectively told people, “Apply and sign and tell us that you’re really entitled to the money,” according to Justice Department Inspector General Michael Horowitz. The SBA camouflaged its “don’t ask, don’t tell” loan standard by claiming to perform economic miracles. The SBA ludicrously boasted that PPP loans saved more jobs than the total number of employees in at least 15 industries.
Yet CBS News found that PPP loans had gone to more than a thousand “ghost businesses” in Markham, Illinois — indicative of a nationwide problem of deluging non-existent companies with federal cash. The feds gave “loans to 342 people who said their name was ‘N/A,’” the New York Times reported.
Fraud permeated relief programs of practically every federal agency that gushered money. On September 20, the feds charged 47 people in Minnesota with looting $250 million from the federal child nutrition programs’ COVID aid. Prosecutors denounced the “brazen scheme of staggering proportions” but federal and state bureaucrats should have stopped the pilfering from the start. “Feeding Our Future,” a nonprofit organization, pocketed $300,000 in subsidies in 2018 and a windfall of almost $200 million in 2021. Fraud snowballed because the US Department of Agriculture issued waivers to “suspend all on-site monitoring of providers” of children’s meals.
Instead of feeding hungry kids, tax dollars were pilfered using a list of phony recipients generated by the website listofrandomnames.com. (No wonder Feeding Our Future wasn’t invited to attend Biden’s White House Summit on Hunger last week.) When the state of Minnesota sought to cut off funding, Feeding Our Future sued, claiming the action “discriminated against a nonprofit that worked with racial minorities,” the Minneapolis Star Tribune reported. Leftist firebrand Rep. Ilhan Omar (D-Minn.) received thousands of dollars in donations from individuals indicted in the scandal.
Fighting fraud is tricky for federal investigators when some politicians openly used COVID stimulus money to bribe voters. In the January 2021 Georgia runoff race for US Senate, the campaign of Democratic candidate Raphael Warnock distributed fliers declaring, “Want a $2,000 Check? Vote Warnock.” That promise helped Warnock win, sealing Democratic control of the Senate and opening the floodgates for trillions of dollars of additional Biden administration spending.
[...]
nypost.com [2022-10-04] James Bovard, October 2, 2022 link archive General
Thousands of officials across the government’s executive branch reported owning or trading stocks that stood to rise or fall with decisions their agencies made, a Wall Street Journal investigation has found.
More than 2,600 officials at agencies from the Commerce Department to the Treasury Department, during both Republican and Democratic administrations, disclosed stock investments in companies while those same companies were lobbying their agencies for favorable policies. That amounts to more than one in five senior federal employees across 50 federal agencies reviewed by the Journal.
A top official at the Environmental Protection Agency reported purchases of oil and gas stocks. The Food and Drug Administration improperly let an official own dozens of food and drug stocks on its no-buy list. A Defense Department official bought stock in a defense company five times before it won new business from the Pentagon.
The Journal obtained and analyzed more than 31,000 financial-disclosure forms for about 12,000 senior career employees, political staff and presidential appointees. The review spans 2016 through 2021 and includes data on about 850,000 financial assets and more than 315,000 trades reported in stocks, bonds and funds by the officials, their spouses or dependent children.
[...]
The vast majority of the disclosure forms aren’t available online or readily accessible. The review amounts to the most comprehensive analysis of investments held by executive-branch officials, who have wide but largely unseen influence over public policy.
AMONG THE JOURNAL’S FINDINGS:
• While the government was ramping up scrutiny of big technology companies, more than 1,800 federal officials reported owning or trading at least one of four major tech stocks: Meta Platforms Inc.’s Facebook, Alphabet Inc.’s Google, Apple Inc. and Amazon.com Inc.
• More than five dozen officials at five agencies, including the Federal Trade Commission and the Justice Department, reported trading stock in companies shortly before their departments announced enforcement actions, such as charges and settlements, against those companies.
• More than 200 senior EPA officials, nearly one in three, reported investments in companies that were lobbying the agency. EPA employees and their family members collectively owned between $400,000 and nearly $2 million in shares of oil and gas companies on average each year between 2016 and 2021.
• At the Defense Department, officials in the office of the secretary reported collectively owning between $1.2 million and $3.4 million of stock in aerospace and defense companies on average each year examined by the Journal. Some held stock in Chinese companies while the U.S. was considering blacklisting the companies.
• About 70 federal officials reported using riskier financial techniques such as short selling and options trading, with some individual trades valued at between $5 million and $25 million. In all, the forms revealed more than 90,000 trades of stocks during the six-year period reviewed.
• When financial holdings caused a conflict, the agencies sometimes simply waived the rules. In most instances identified by the Journal, ethics officials certified that the employees had complied with the rules, which have several exemptions that allow officials to hold stock that conflicts with their agency’s work.
[...]
wsj.com [2022-10-14] Rebecca Ballhaus, Brody Mullins, Chad Day, John West, Joe Palazzolo, James V. Grimaldi, Oct. 11, 2022 link archive General
Some sold in January 2020 when the government began mobilizing against the threat. Others bought shares as a market-rescue plan was taking shape.
Federal officials working on the government response to Covid-19 made well-timed financial trades when the pandemic began—both as the markets plunged and as they rallied—a Wall Street Journal investigation found.
In January 2020, the U.S. public was largely unaware of the threat posed by the virus spreading in China, but health officials were on high alert and girding for a crisis.
[...]
wsj.com [2022-10-20] Rebecca Ballhaus, Joe Palazzolo, Brody Mullins, Chad Day John West, Oct 19, 2022 link archive General
In a shocking new report from the Wall Street Journal, leading health officials began offloading stocks at truly unprecedented rates in January 2020—well before the COVID-19 emergency was declared—with officials at the US Department of Health and Human Services selling 60% more stocks in January 2020 than average over the previous 12 months.
One deputy to NIAID Director Anthony Fauci reported selling between $157,000 and $480,000 in stocks before the end of January.
Weeks later, stock prices around the world went into freefall at the fastest rate since the Great Depression as word got round that officials were planning a complete shutdown of the global economy.
The ensuing lockdowns were unprecedented in the western world prior to Xi Jinping’s lockdown of Wuhan and weren’t part of any democratic country’s pandemic plan. They weren’t given any official imprimatur as western policy until February 24, 2020, when WHO Assistant Director-General Bruce Aylward—famous for later disconnecting a live interview when asked to acknowledge Taiwan—reported back about Wuhan’s lockdown from Beijing:
What China has demonstrated is, you have to do this. If you do it, you can save lives and prevent thousands of cases of what is a very difficult disease.
That leading officials were already privately planning to recreate China’s lockdowns across the western world by January 2020, however—and making stock trades based on those plans—further confirms the all-too-prescient stock tip by someone who claimed to have “friends and family in the medical industry and field, including at CDC and one close friend at WHO” on January 30, 2020, which proved to be a near-perfect foretelling of subsequent events:
There are very high profile investors who've been silently pulling out ahead of time… the WHO is already talking about how ‘problematic’ modeling the Chinese response in Western countries is going to be, and the first country they want to try it out in is Italy. If it begins a large outbreak in a major Italian city they want to work through the Italian authorities and world health organizations to begin locking down Italian cities in a vain attempt to slow down the spread at least until they can develop and distribute vaccines, which btw is where you need to start investing.
michaelpsenger.substack.com [2022-10-20] Michael P Senger, Oct 19, 2022 link archive General
AHIP Study Finds Top Drug Companies’ Sales and Marketing Budgets Swamp R&D Budgets
In case you missed it, America’s Health Insurance Plans (AHIP) released a new study Wednesday that found Big Pharma continued to spend more advertising and selling its products than investing in research and development (R&D) even amid unprecedented focus on the development of new treatments as a result of the COVID-19 pandemic.
The study found that “Of the 10 drug manufacturers examined, 7 of them spent more on selling and marketing expenses than they did on research and development. For this group of 10 companies alone, selling and marketing expenses exceeded R&D spending by $36 billion, or 37%.” AHIP emphasized that, “this use of dollars occurred during a year dedicated to the development of new treatments and vaccines to overcome the COVID-19 crisis.”
The study shows that brand name drug manufacturers including AbbVie, Pfizer, Novartis, GlaxoSmithKline, Sanofi, Bayer and Johnson & Johnson all spent more on marketing and selling their products in 2020 than they did on developing new treatments:
AbbVie spent $11 billion on sales and marketing in 2020, compared to $8 billion on R&D.
Pfizer spent $12 billion on sales and marketing, compared to $9 billion on R&D.
Novartis spent $14 billion on sales and marketing, compared to $9 billion on R&D.
GlaxoSmithKline spent $15 billion on sales and marketing, compared to $7 billion on R&D.
Sanofi spent $11 billion on sales and marketing, compared to $6 billion on R&D.
Bayer spent $18 billion on sales and marketing, compared to $8 billion on R&D.
Johnson & Johnson spent $22 billion on sales and marketing, compared to $12 billion on R&D.
“Big Pharma’s practices clearly show that their growth strategy is based on selling a greater volume of drugs to patients – not on creating groundbreaking new therapies and delivering more value to patients,” AHIP wrote, concluding that, “With thoughtful solutions that encourage private-market competition and end pharma’s gaming of the system, we can have both.”
The COVID-19 crisis presented ripe opportunities for fraudsters and swindlers to exploit the system.
The COVID-19 pandemic, which placed unprecedented demands on federal financial assistance programs, also presented ripe opportunities for fraudsters and swindlers to exploit the system.
A report released by the Department of Justice (DOJ) COVID-19 Fraud Enforcement Task Force uncovered a shocking scope of fraud during the pandemic, with over $400 billion in emergency funding either stolen or misappropriated.
According to the report, fraudulent claims and schemes targeted various pandemic relief efforts, including unemployment insurance benefits, Paycheck Protection Program (PPP) loans, and Economic Injury Disaster Loans (EIDLs), among others.
These included fraudulent claims filed using stolen identities, inflated payroll expenses, doctored bank statements, and false tax forms.
The report reveals that fraudsters and swindlers may have stolen upwards of $280 billion in emergency funding, with an additional $123 billion lost or misappropriated, totaling more than $400 billion in funds intended to aid Americans during one of the most challenging times in recent history, The Politics Brief reported.
Here are some examples of COVID-19 fraud cases:
A defendant was sentenced to seven years in federal prison for committing PPP, EIDL, and UI fraud, with actual losses of more than $1 million and attempted losses of $3 million. When the government executed search warrants in the case, agents recovered stolen identifying information and ghost guns, including one modified to function as a machine gun.
A defendant pleaded guilty to submitting more than $3.5 million in fraudulent COVID-19 PPP and EIDL applications and using fraudulently obtained funds to pay for a vacation, a Mercedes-Benz, jewelry, and luxury goods, including items from Luis Vuitton, Neiman Marcus, Dior, Cartier, Gucci, Chanel, and Hermes.
The SDFL indicted 17 employees of the Broward Sheriff’s Office were charged with obtaining fraudulent PPP/ EIDL loans. One former deputy was recently convicted at trial, several employees have pleaded guilty, and other defendants’ cases are still pending.
A defendant was sentenced to 71 months in prison for fraudulently obtaining PPP and EIDL loans and Shuttered Venue Operator Grants (SVOG), using the stolen funds to buy two Tesla S models, a Lamborghini, a Porsche, a diamond Audemars Piguet watch, a rose gold and diamond pendant with his company’s logo, a half-kilogram gold chain with 70 carats of diamonds, and a 1-kilogram gold chain.
A former contract detention officer at the federal Krome Detention facility who was the leader of a PPP fraud ring was sentenced to 32 months in prison for preparing fraudulent PPP applications in return for kickbacks.
A defendant was sentenced to 70 months in prison for laundering the over $2 million in fraudulently obtained PPP and EIDL loans and using the funds to gamble and to pay for cosmetic surgery, a Cadillac Escalade, and a Pomeranian puppy.
In the Southern District of Georgia, a Florida-based attorney was convicted at trial of conspiracy to fraudulently obtain almost $800,000 in Economic Injury Disaster Loans for herself and others.
In the Western District of Washington, the ringleader of a $6.8 million pandemic fraud ring was sentenced to five years in prison for fraudulently seeking funds from various relief programs.
In the Eastern District of Washington, an Arkansas-based business owner pleaded guilty to fraudulently receiving more than $16.5 million in SBApandemic relief funds for himself and others.
In the Eastern District of Virginia, a former VA nurse was sentenced to 18 years in prison for conspiring to fraudulently obtain more than $3.5 million in UI benefits from at least five states. She and her co-conspirators filed more than 220 false applications for unemployment insurance benefits using stolen identities and the identities of state and federal prison inmates.
In the Middle District of Florida, a defendant was sentenced to eight years and six months in prison for obtaining more than $7.2 million in PPP loan funds, which he used to purchase Maserati and Mercedes-Benz cars and buy a 12-acre estate.
The District of Minnesota has brought charges against more than 50 individuals for their respective roles in a $250 million fraud scheme that exploited a federally funded child nutrition program during the COVID-19 pandemic.
In the Eastern District of Michigan, a man was sentenced to 15 years in prison for his role as the ringleader of conspiracies to use stolen identities to fraudulently obtain $2.1 million in unemployment insurance benefits from multiple states and to traffic in methamphetamine.
The DOJ’s COVID-19 Fraud Enforcement Task Force has made significant strides in combating this fraud, with over 3,500 defendants criminally charged with more than $1.4 billion in fraudulently obtained CARES Act funds seized or forfeited and more than 400 civil settlements and judgments.
However, the sheer magnitude of the fraud indicates that much work remains to be done.
[...]
vigilantnews.com [2024-04-11] Jim Hoft, April 10, 2024 link archive General
“He’s not a doctor; he’s not a virologist. He’s not even a college graduate.”
The world’s richest college dropout and Co-founder of Microsoft, Bill Gates, has a peculiar record of making lucrative investments. The timing of these moves is repeatedly so impeccable that people often ask, “How did he know?”
For example, Bill Gates invested in BIOMILQ in 2020, a startup aimed at producing human breast milk in a lab. Coincidentally, milk production issues are a side effect of C19 inoculation — and a baby formula shortage has also plagued America.
And what may be most notable is Bill Gates’ $55 million investment in BioNTech in 2019 — before just about anyone knew a thing about mRNA technology or COVID-19. That turned out to be a substantial payout, as that $55 million grew tenfold to over $550 million in just two years.
And he secured the bulk of that profit, offloading 86% of his shares held in the most profitable quarter (Q3 2021).
After making hundreds of millions from mRNA technology, Bill Gates is now trashing the C19 jabs, advocating for an inhaled solution instead — which makes one ask, “Are you invested in that?”
NOW — Bill Gates Trashes Current COVID Jabs But Teases New Option
“We think you can have…a thing that you can inhale that will mean you can’t be infected — an inhaled blocker.
The current vaccines are not infection blocking, they’re not broad, & they have very short duration.” pic.twitter.com/lSk8PZfiaA
So, investment after investment, Bill Gates is making BIG money while Americans and the world are going through adversity. Is he the Nostradamus of our time? Perhaps the luckiest man ever? Or is there something else going on with his impeccable timing?
Jimmy Dore certainly has a viewpoint on the matter.
False positive cases nearly cost us our society. Hospitals cashed in, to the tune of $250,000 dollars per COVID-19 hospitalization - far more than needed.
In March 2023, The New York Times published this image showing that $483 billion of government aid had been spent to bail out big medicine. Right off the bat, we see $64 billion was wasted on vaccines that do not prevent transmission and only look like they reduce COVID-19 severity if you ignore COVID-19 cases for 8 weeks after the first exposure.
Given the shell-and-pea game of reimbursements, cost-sharing, Medicaid and Medicare and COBRA payments to healthcare providers totaled $125 Billion - on top of the $156 paid directly to healthcare providers for a grand total of $281 Billion.
There are about 920 thousand (corrected from million) hospital beds in the United States, and not all beds were used for COVID-19. According to NPR, only 1/5 of hospital beds were dedicated to COVID-19 beds. That means at least $1.5M were given to hospitals per COVID-19 hospital bed.
But that’s a pittance. According to the AHA, in March 2021, $1.9 Trillion were actually allocated to Big Medicine under a "Relief Reconciliation" scheme - basically a bail-out of nearly every aspect of Big Medicine… to make up for insufficient compensation to healthcare providers.
The AHA complained there was no relief in the Relief Reconciliation to healthcare providers… yet via indirect compensation, all hospital costs were clearly programmed for overcompensation.
According to this published report reported costs per patients, however, were at most $50,000 (and that's for ventilated patients). At the low-end costs were $14K per patient.
CDC estimates there have been 7.5 million COVID-19 hospitalizations. Given the $1.9 Trillion dollar bail-out, each hospitalization cost the US $250,000, at least five times and more frequently ten times the amount of money required.
Admittedly these are general analyses that oversimplify. Still, I’ve said since 2015 medicine for profit is an unsustainable model. Let’s not call bail-outs of big medicine “Relief Reconciliation”. They are bailouts of an unsustainable business.
Big Medicine is unsustainable at any scale - meaning if we all get sick more often, the problem will get larger.
[...]
popularrationalism.substack.com [2023-06-16] James Lyons-Weiler, June 14, 2023 link archive General
The world has been counting on the intelligence community to call out anything untoward about the response to COVID. Of course, that won’t happen, because they’re the ones who planned it.
From an early date, commentators have noted that the response to COVID had all the look and feel of a coup attempt. The masks, the slogans, the symbols, the lies, the sudden inversion of long-cherished norms and values, the mindless acceptance of information from nefarious sources like the World Health Organization and China. Something was seriously off, and it all seemed so obvious.
Thus, one overarching question always lingered over the response to COVID. How were officials able to implement such destructive, totalitarian policies across the western world without intelligence authorities stepping in to stop them?
A detached review of the evidence leads to a chilling answer—though in hindsight, perhaps the only one that was ever really possible. Quite simply, the reason the western intelligence community never stepped in to stop this illiberalism is that virtually all the most illiberal aspects of the response to COVID lead directly back to the western intelligence community itself.
Reviewing the Evidence
[...]
Additional references:
Pandemic Simulations
Operation Dark Winter
Event 201
Michael Callahan
Matthew Pottinger
Deborah Birx
Li Wenliang
michaelpsenger.com [2023-08-03] Michael P Senger, August 1, 2023 link archive General
<The transcript has not been edited as carefully as I could for grammatical mistakes, with some clarifications and reduction in unnecessary text - so hopefully it isn’t too cringe worthy. RWM>
Veronika Kyrylenko: Hi everyone. This is Veronica Kyrylenko with the New American magazine. We're in Madison Virginia, where we're hosted by Dr. Robert Malone, a brilliant scientist and the original inventor of mRNA vaccine technology, turned freedom fighter and a fearless troublemaker, taking on the deep state now.
Dr. Malone, just as the memory of COVID was beginning to fade from the public minds, like a haunting nightmare with occasional reminders caused by painfully slow congressional hearings regarding the Bethesda Boys and their knowledge timeline, you sir, inadvertently dropped a nuclear truth bomb. You aimed not at the regular usual suspects like the NIH technocrats that were practically caught red-handed in Wuhan. You sir, aimed not at the DOD that had its own shady dealings and business with the Wuhan lab.
Now, Dr. Malone, you aimed at Langley. While speaking with Steve Bannon last week, you said quoting your sources from inside the CIA,
"Clearly the United States intelligence community was at the heart of this whole COVID crisis, working together with the CCP throughout this entire affair."
So first of all, let's set the records straight and focus on the first part of your statement. What do you mean, the intelligence community was at the heart of this whole COVID crisis? Which role exactly did our intelligence community play before and during the pandemic?
Dr. Robert Malone: When I speak of the intelligence community, it's a very broad spectrum of capabilities that includes the Department of Defense activities, under Tony Fauci, as it also includes the NIH (biodefense research activities). And then, it's even larger than that because of the Five Eyes Alliance. So this is Great Britain or UK, Canada, US, Australia and New Zealand; all the lockdown countries that have been perhaps most aggressive in their propaganda, use of fifth generation warfare, the censorship, retaliation against civilian populations, et cetera.
So when I speak of the intelligence community, I'm really talking about a matrix of capabilities that are global, that knowledgeable people within my sphere argue is the most powerful organization on earth. That currently, full stop, has amazing global reach. Obviously, the intelligence community has no moral compunctions about manipulating elections, assassination of foreign leaders or a number of other activities that most of us would consider to be unethical. But these are justified as necessary or supportive of the interests of this kind of imperialistic world that we live in right now.
With the desire by leading economic powers and their surrogates and governmental organizations to gain power and control over resources and all kinds of things. Even to the level that various speakers representing the World Economic Forum and the United Nations use language like “we own the science”. So I'm talking about the entire matrix.
[...]
What has been their role throughout this COVID crisis? [...] For me, I've had this journey of discovery. For instance, through Ernst Wolff's thinking, that a lot of this was driven by an economic agenda and manipulated by various economic forces. Many people assert that the central banks and the Bank of International Settlements has been the puppet master behind all of this. And there's various theories that have been floated that it was old European royalty, that it was the British crown, that it was the cabal of central banks, that it was, as I mentioned, the BIS (Bank of International Settlements), that it was the WEF, or that it was the CCP. That it was the CCP has been the initial thesis that was promoted so aggressively by many people. That this was all the CCP pulling the strings of the West. I have been really reluctant and yet also criticized for imagining that the United States government had a major role in this.
[...]
So there's some things that have really bothered me all the way through this. One was having the opportunity to hear and interact directly with Michael Callahan early on in the outbreak. He said a series of things. Michael Callahan being a retired CIA officer who was at DARPA, who was a program officer responsible for a lot of the modern biologics programs.
[...]
So to recap, Callahan gave me a call on January 2nd of 2020, in which he told me that this virus, while he was in Wuhan at the time <that was what he told me>, that there was this coronavirus that looked like a real threat. That it had emerged into the population in Wuhan and that I should get the people that I've been associated with loosely (for years) activated and focused on trying to come up with potential solutions for this in terms of medical countermeasures- drugs or vaccines- for this new coronavirus that had emerged in Wuhan.
[...]
I had downloaded this “Wuhan seafood market virus” sequence from the NIH sequence database as soon as it was released, which I think was January 10th or January 11th, and started working on modeling x-ray crystallography based on that sequence, et cetera, so we could work on computational drug discovery (to discover repurposed drugs with anti-viral properties). And I had a series of conversations with Michael on and off.
He shared with me what he was doing at various points in time (early in the pandemic). For instance, he was on point for the Diamond Princess outbreak. At the time, I was directly interacting with passengers on the Diamond Princess and learning from them what was going on. He was on point for the design and deployment of the tent hospitals in New York City, and he was on point for development of the protocols and management of the elder care facilities throughout the United States beginning in the West Coast. So those are three kind of key things in the timeline of COVID. In February 2020, I challenged him:
"Michael, this seems like it was a engineered virus that came from the laboratory, this laboratory Wuhan Institute-"
The line between being overly cautious and just plain cruel has been crossed repeatedly. This is where we are today in what had previously been thought of as civilization:
Hospitals across the country are removing unvaccinated organ transplant patients from waiting lists. Medical ethicists are fine with this, because the patients need to be protected from illnesses while their bodies accept the new organs, and they are prioritized based on their chances of survival. These “ethicists,” however, come off as vindictive, “othering” the unvaccinated in line with the narrative. Moving these patients lower on the list based on a risk they assume seems acceptable, dropping them altogether is not. It’s intentionally punitive and ghoulish. The decisions reinforce, as well, the naked fact that the vaccine mandates are authoritarian power plays.
A Virginia hospital that refused to provide Ivermectin prescribed by a doctor to a dying COVID patient was found in contempt of court before it finally relented and allowed the drug to be administered. It was too late, though. The woman died five days after the judge’s ruling.
At Georgetown University, “fully vaccinated students are randomly tested for COVID each week,” the Daily Mail reported last month, “and even those who are asymptomatic are ordered to stay in a room in a designated building where they spend 10 days in confinement.”
[...]
issuesinsights.com [2022-02-10] February 9, 2022 link archive General
Throughout wave after wave of COVID-19, a range of voices have called for reforming the way governments manage pandemics. From mixed messages to inequitable vaccine distribution, the global response to COVID-19 just hasn’t cut it. In particular, critics have highlighted the World Health Organization (WHO) as a primary target for reform efforts, and, by now, several groups inside and outside of the organization have begun developing proposals that range from reforming the WHO to developing whole new international forums specifically designed to prepare for and mount an effective pandemic response.
Last December, at a special meeting of the World Health Assembly, the governing body of the WHO, country representatives agreed to kick off reforms when they voted for negotiating an international agreement or pandemic treaty. With the vote, the conversation seemingly moved beyond simply reforming the WHO and towards the creation of a stand-alone legally binding instrument: a new international structure to address pandemics.
Pandemics could become more frequent in the years to come as the world grows even more interconnected, increased agricultural production leads to more contact between humans and animals with the potential for further spread of zoonotic diseases, and humans encroach further into wildlife areas. While an international pandemic organization sounds important in theory, organizations like the UN Security Council can’t necessarily solve the problems they were intended to solve. Creating a new pandemic response system will likely require years of difficult negotiations and could still result in a structure unable to forcefully respond to an outbreak, or an agreement supported by only some countries and perhaps not all of the key global leaders. By looking at the reform ideas that people and organizations have put forward, one can begin to see the contours of what a new global response system might look like.
Who gets to decide when emergency powers are authorized A governor? The President? The Senate? Congress? The director of the WHO? When and how do those powers end? Obviously, what is happening is a slippery slope.
Unfortunately, much of this pending legislation at the international level has been kept out of the public eye and is not readily transparent or available to be analyzed. Furthermore, the media is not doing its job in making these pending public policy measures available for people to assess for themselves.
thebulletin.org [2022-04-10] By Daniel Gerstein, April 1, 2022 link archive General
This analysis piece will attempt to examine some of the critical pandemic-related measures implemented in the United States from an immunological perspective and pinpoint caveats that should have been considered before their implementation. I also discuss alternative measures grounded in scientific data that were not thoroughly explored and likely could have helped fight the pandemic.
[...]
5. Alternative Measures to Vaccines to Fight the Pandemic
Bias towards vaccines as the single most crucial tool to fight the pandemic was evident from the beginning. However, these vaccines do not prevent infections and provide little protection from long COVID [72], and even if we succeeded in injecting the entire world population, we would have likely put an even stronger evolutionary pressure on the virus to mutate and evade the immune responses triggered by the vaccine. The best example of how non-sterilizing vaccines can lead to more pathogenic variants is the vaccine generated to fight Marek disease in poultry [73,74]. This caveat and those discussed above highlight the lack of a solid scientific rationale to focus on vaccines targeting a single viral component. We have been fighting influenza for decades. Influenza induces short- and long-term symptoms and kills people in a similar way to COVID, and the same target population is at risk [75,76,77,78,79,80,81]. We have a standard of care in place with influenza symptoms and other respiratory diseases, some of which could have been better used to treat COVID.
Efforts to repurpose drugs with high safety profiles could have been better supported and managed. Drug repurposing and developing novel therapeutics to treat COVID have been reviewed elsewhere [82]. Here, I will briefly discuss the efforts to repurpose two drugs, chloroquine (alone, or its hydroxy derivate, or combined with azithromycin) and remdesivir, to highlight possible concerns on how drugs become classified as effective by regulatory agencies. Chloroquine, hydroxychloroquine, and azithromycin are cheap and safe drugs taken by millions around the world daily for different inflammatory diseases and malaria. After some promising data on the use of these drugs to treat COVID [83], follow-up clinical trials failed to show their benefits in fighting COVID [84,85,86]; therefore, they were not implemented as the standard of care in Western countries. Chloroquine/hydroxychloroquine/azithromycin/ivermectin are still the primary go-to drugs in low-mortality-rate African countries to prevent and treat COVID [87,88,89,90]. Whether the low mortality rate in these countries is due to the use of these drugs or other factors, such as vaccination history [91,92,93], age, etc., remains to be determined [90]. In contrast, the previously untested remdesivir was fast-tracked and adopted as the standard of care despite opposing clinical trial outcomes [94]. One well-designed but maybe underpowered clinical trial did not reveal any statistically significant clinical benefits of remdesivir for treating severe COVID [95,96], and neither did the WHO Solidarity Trial [97]. In contrast, The National Institute of Allergy and Infectious Diseases (NIAID)-sponsored, somewhat controversial trial [98] found that remdesivir slightly reduced the duration of the disease (from 15 days to 11 days), though not mortality from COVID [99,100]. However, the already questionable benefits of using remdesivir might be even further diminished by reports of kidney and liver toxicity [101].
The monoclonal antibody therapy targeting the SARS-CoV-2 spike protein from Regeneron and others became available early in the pandemic. It was shown to be highly effective in preventing the development of severe illnesses and hospitalization without any significant side effects. This treatment option, which can now be easily administered subcutaneously [102], could likely have been made available to anyone who needed it for a fraction of the total vaccine costs.
Early research showed that patients with severe COVID had low levels of vitamin D [103,104,105]. People with dark skin need more sunlight than people of Northern European ancestry to generate similar amounts of vitamin D, and they are disproportionally affected by COVID [106,107,108]. Therefore, simple lifestyle adjustments that involve nutrition, exercise, and supplements should probably have been implemented as a preventative measure against COVID. These measures would likely also constitute a long-term general solution for achieving a much healthier population that is more resistant to infections and chronic diseases.
[...]
7. Layman’s Summary
The virus fatality rate did not support lockdowns, blanket restrictive measures, and non-selective mass vaccinations. There was no solid scientific rationale to adopt the untested mRNA-LNP platform over other well-established vaccine formulations to fight COVID. Scientists, experts, government officials, the media, and scientific journals, all contributed to suppressing alternative ideas on how to manage the pandemic. Some of these groups are still promoting the scientifically debunked idea that the present vaccines protect you from catching COVID and becoming sick [116], and that this is a pandemic of the unvaccinated [117]. Unfortunately, the virus is likely here to stay in one form or another, and we must learn to live with it. How effective the lockdowns and other restrictive measures were in reducing COVID deaths are still a matter of debate [118,119,120,121], but we likely lost, or we will lose a lot more people, from the direct and indirect effects of these measures. The excess of global deaths is often exclusively attributed to COVID [122]. However, these reports fail to factor in the direct and indirect effects of COVID-related restrictions. Many people died because they did not have access to healthcare during this period (they were afraid of going to the hospitals, or the hospitals did not accept them). Furthermore, a significant increase in suicide rates, drug and alcohol abuse, domestic violence, obesity, economic hardships, vaccination-related events, etc., likely contributed to excess deaths. If the vaccines do not prevent infections and spread, it is time to stop coercing people to get vaccinated, vilifying unvaccinated people, and giving extra perks to the vaccinated. It is neither feasible nor economically sustainable to “vaccinate” everyone every few months or perform continuous testing, and more importantly, there is no scientific rationale for doing so. We must focus our resources on the vulnerable population and provide them with efficient treatment options and possible preventative steps in the form of lifestyle changes, supplements, and effective, long-lasting, safe, and affordable vaccines.
[...]
ncbi.nlm.nih.gov [2022-08-27] Botond Z. Igyártó, July 20, 2022 link archive General
Bret speaks with Norman Fenton on the failure of academia and our medical system that Covid has revealed. They discuss how Wikipedia, the greatest encyclopedia to date, has become a political weapon, and how big an issue this actually is.
The CDC’s fall from grace around the Covid Pandemic Response, brings into focus years of fraud plaguing Science and Public Health. With claims of misconduct, and bad research behavior going back decades, some top Officials believe up to HALF of all scientific literature may be untrue.
There is perhaps no bigger plausibility sham today than “evidence-based medicine” (EBM). This term was coined by Gordon Guyatt in 1990, after his first attempt, “Scientific Medicine,” failed to gain acceptance the previous year. As a university epidemiologist in 1991, I was insulted by the hubris and ignorance in the use of this term, EBM, as if medical evidence were somehow “unscientific” until proclaimed a new discipline with new rules for evidence. I was not alone in criticism of EBM (Sackett et al., 1996), though much of that negative response seems to have been based on loss of narrative control rather than on objective review of what medical research had actually accomplished without “EBM.”
[...]
Conclusions
Many other instances of plausible scientific claptrap or bad science have occurred during the Covid-19 pandemic. As was seen with the retracted Surgisphere papers, medical journals routinely and uncritically publish this nonsense as long as conclusions align with government policies. This body of fake knowledge has been promulgated at the highest levels, by the NSC, FDA, CDC, NIH, WHO, Wellcome Trust, AMA, medical specialty boards, state and local public health agencies, multinational pharma companies and other organizations around the world that have violated their responsibilities to the public or have purposely chosen not to understand the fake science.
The US Senate recently voted, for the third time, to end the Covid-19 state of emergency, yet President Biden stated that he would veto the measure because of “fear” of recurring case numbers. My colleagues and I argued almost a year ago that the pandemic emergency was over (Risch et al., 2022), yet the spurious reliance on case counts to justify suppression of human rights under the cover of “emergency” continues unabated.
Massive censorship by the traditional media and much of social media has blocked most public discussion of this bad and fake science. Censorship is the tool of the undefendable, since valid science inherently defends itself. Until the public begins to understand the difference between plausibility and science and how large the effort has been to mass-produce science “product” that looks like science but is not, the process will continue and leaders seeking authoritarian power will continue to rely on it for fake justification.
brownstone.org [2022-12-01] Harvey Risch, November 26, 2022 link archive General
Trend Over Last Few Years Indicates Fear of the Truth Amongst Vaccine Promoters
[...]
Hotez is now joined by Tedros at the WHO and Fauci (retired NIH) in promulgating the term anti-science as a pejorative and insulting way of positioning clinical scientists who are studying the epidemiology, pathophysiology, and clinical consequences of COVID-19 vaccine injuries, disabilities, and deaths. Yes, the study of what COVID-19 vaccines do to the human body is “science” and it is insulting to hear the term “anti-science” thrown out as a blocking tool in order to discount any side effects of vaccination.
Tedros went so far as to say those studying vaccine injuries and who wisely chose to defer on vaccination themselves are “killing machines.” This unhinged hyperbole is symptomatic of a psychotic break in those who who have been the vanguard of the imploding worldwide narrative supporting mass vaccination.
I summarized these comments and pivoted on television to the opportunities that Drs Fauci, Walensky, Jha, Murthy, and several others had on Jan 24 and Dec 7, 2022, to attend US Senate Hearings and listen to COVID-19 experts and have an interchange on the “science” of what we have learned. Instead none of them showed up and now are painting themselves with the term “anti-science”. This regression can only lead to greater loss of credibility and dissolution of the crumbling false narrative “safe and effective.”
[...]
See related data element: Anti-science extremism in America: escalating and globalizing
petermcculloughmd.substack.com [2022-12-25] Peter A. McCullough, MD, MPH™, December 24, 2022 link archive General
Background: The COVID-19 period highlights a huge problem that has been developing for decades, the control of science by industry. In the 1950s, the tobacco industry set the example, which the pharmaceutical industry followed. Since then, the latter has been regularly condemned for illegal marketing, misrepresentation of experimental results, dissimulation of information about the dangers of drugs, and considered as criminal. Therefore, this study was conducted to show that knowledge is powerfully manipulated by harmful corporations, whose goals are: 1/financial; 2/to suppress our ability to make choices to acquire global control of public health.
Methods: Pharmaceutical industry techniques for manipulating science and COVID-19 reporting were reviewed. Several sources of official documents were used: PubMed; National Institutes of Health resources; pharmaceutical companies; policy documents; national newspapers and news agencies; and books by prominent professionals (scientific and legal). A few studies have not been published in peer-reviewed journals; however, they have been conducted by reputable scientists in their respective fields.
Results: Since the beginning of COVID-19, we can list the following methods of information manipulation which have been used: falsified clinical trials and inaccessible data; fake or conflict-of-interest studies; concealment of vaccines' short-term side effects and total lack of knowledge of the long-term effects of COVID-19 vaccination; doubtful composition of vaccines; inadequate testing methods; governments and international organizations under conflicts of interest; bribed physicians; the denigration of renowned scientists; the banning of all alternative effective treatments; unscientific and liberticidal social methods; government use of behavior modification and social engineering techniques to impose confinements, masks, and vaccine acceptance; scientific censorship by the media.
Conclusion: By supporting and selecting only the one side of science information while suppressing alternative viewpoints, and with obvious conflicts of interest revealed by this study, governments and the media constantly disinform the public. Consequently, the unscientifically validated vaccination laws, originating from industry-controlled medical science, led to the adoption of social measures for the supposed protection of the public but which became serious threats to the health and freedoms of the population.
Republicans in the New Hampshire House united this week to pass multiple bills dealing with COVID-19, with a focus on prioritizing individual rights and limiting the authority of entities to compel adherence to public health policies.
The action by the House moves the debate over COVID policy to the state Senate, which has so far heard far fewer bills related to the pandemic than the House. In fact, questions of masking, vaccines, and the reach of government have been on the front burner for House lawmakers all year.
[...]
The most high-profile bill, sponsored by House Speaker Sherman Packard, would bar the state from enforcing federal vaccine mandates. Before that proposal was voted through along near party lines. Rep. Mark Pearson of Hampstead, who is chair of the House Health and Human Services Committee, asked colleagues to recognize there is a long tradition of states bucking federal laws.
“In the 19th century, some northern states passed individual liberty laws, which made it illegal for citizens of their states to help enforce the Fugitive Slave Act,” Pearson said.
The House also voted to outlaw mask mandates in public schools (H.B. 1131), and to give the Legislature final say over any decision by the state’s health commissioner to add a vaccine to the list of required inoculations for children (H.B. 1379).
[...]
nhpr.org [2022-04-10] By Josh Rogers, March 17, 2022 link archive General
Asking someone about their shot status could become a crime in Louisiana as lawmakers debate a bill targeting "vaccine discrimination" in the wake of the COVID-19 pandemic.
House Bill 54 by Republican Rep. Larry Bagley of Stonewall would prohibit barring anyone from entering a business, government office or home based on his or her vaccine status.
"I think as an American citizen it's my right to choose what I put in my body (without fear of discrimination)," Bagley said as he presented his bill to the House Criminal Justice Committee Thursday.
[...]
theadvertiser.com [2022-04-10] Greg Hilburn, March 24, 2022 link archive General
We need to be careful to avoid declaring victory over Covid tyranny. You may have thought that with the worldwide protests against mask mandates and lockdowns, and the deaths attributable to the vaccine poisons, our enemies would at least give us a break. But of course they’re not. They are planning a new fake “Covid wave” with more lockdowns, mask mandates, and deadly vaccines. In short, global tyranny.
Information is coming in all the time about the criminal folly of brain-dead Biden and “Dr. Death” Fauci’s policy. For example, a renowned oncologist, Dr. Angus Dalgleish, wrote an open letter to a leading British medical journal warning that the vaccines cause cancer: “Dr. Angus Dalgleish, a renowned oncologist practising in the UK, recently wrote an open letter to the editor-in-chief of the medical journal The BMJ, urging the journal that harmful effects of Covid injections be ‘aired and debated immediately’ because cancers and other diseases are rapidly progressing among ‘boosted’ people.
Dr. Dalgleish is a Professor of Oncology at St George’s, University of London. His letter to Dr. Kamran Abbasi, the Editor in Chief of the BMJ, was written in support of a colleague’s plea to Dr. Abbasi that the BMJ make valid informed consent for Covid vaccination a priority topic.
Covid no longer needs a vaccine programme given the average age of death of Covid in the UK is 82 and from all other causes is 81 and falling.
The link with clots, myocarditis, heart attacks and strokes is now well accepted, as is the link with myelitis and neuropathy. (We predicted these side effects in our June 2020 QRBD article Sorensen et al. 2020, as the blast analysis revealed 79% homologies to human epitopes, especially PF4 and myelin.)
However, there is now another reason to halt all vaccine programmes. As a practising oncologist I am seeing people with stable disease rapidly progress after being forced to have a booster, usually so they can travel.
Even within my own personal contacts I am seeing B cell-based disease after the boosters. They describe being distinctly unwell a few days to weeks after the booster – one developing leukaemia, two work colleagues Non-Hodgkin’s lymphoma, and an old friend who has felt like he has had Long Covid since receiving his booster and who, after getting severe bone pain, has been diagnosed as having multiple metastases from a rare B cell disorder.
I am experienced enough to know that these are not the coincidental anecdotes that many suggest, especially as the same pattern is being seen in Germany, Australia and the USA.
The reports of innate immune suppression after mRNA for several weeks would fit, as all these patients to date have melanoma or B cell based cancers, which are very susceptible to immune control – and that is before the reports of suppressor gene suppression by mRNA in laboratory experiments.
This must be aired and debated immediately.
[...]
lewrockwell.com [2022-12-15] Llewellyn H. Rockwell, Jr., Dec 12, 2022 link archive General
The World Health Organization has already begun drafting a global pandemic treaty on pandemic preparedness. What form will it take? What teeth will it have? How will it further the globalists in cementing the biosecurity grid into place? James breaks it down in today's episode of The Corbett Report podcast.
The Lancet Commission on the coronavirus pandemic has delivered a harsh verdict on how the world responded — it was “a massive global failure,” the prestigious journal declared. Governments were too slow and cautious, faced deep public mistrust, were undermined by misinformation and failed to serve the most vulnerable. “The result was millions of preventable deaths,” the Lancet said. This sorry record must provide impetus to do better in the future.
The Lancet convened 28 experts under Columbia University’s Jeffrey Sachs for a two-year examination of pandemic preparedness, response and recovery, delving into public health, virology, social policy, economics, finance and geopolitics. The report is but one of several worthy efforts to draw lessons from the gravest public health disaster in a century. The authoritative new findings deserve attention, though we wish Congress and the White House had ordered a comprehensive, 9/11 Commission-like national panel in the United States. They did not.
A major lesson is that when a highly infectious disease breaks out in a vulnerable population, rapid response is essential, and even more so when many infections are asymptomatic, as was the case with covid-19. A single new case became thousands within a month. “The ability of the public health system to identify cases, trace contacts, and isolate infected individuals can be overwhelmed in just a few weeks of uncontrolled community transmission,” the report says. That’s what happened, over and over. “National responses were often improvisational, occasionally bordering on the absurd,” the commission states. “Several national leaders made highly irresponsible statements in the first few months of the outbreak, neglecting scientific evidence and needlessly risking lives with a view to keeping the economy open.” Governments “showed themselves to be untrustworthy and ineffective,” and “rancor among the major powers” then “gravely weakened the capacity of international institutions” to respond, especially the World Health Organization, which comes in for sharp criticism for repeatedly erring “on the side of reserve rather than boldness.” The panel calls for strengthening the WHO and giving it stronger powers and more solid financing.
Here are the 10 biggest falsehoods—known for years to be false, not recently learned or proven to be so—promoted by America's public health leaders, elected and unelected officials, and now-discredited academics:
1. SARS-CoV-2 coronavirus has a far higher fatality rate than the flu by several orders of magnitude.
2. Everyone is at significant risk to die from this virus.
3. No one has any immunological protection, because this virus is completely new.
4. Asymptomatic people are major drivers of the spread.
5. Locking down—closing schools and businesses, confining people to their homes, stopping non-COVID medical care, and eliminating travel—will stop or eliminate the virus.
6. Masks will protect everyone and stop the spread.
7. The virus is known to be naturally occurring, and claiming it originated in a lab is a conspiracy theory.
8. Teachers are at especially high risk.
9. COVID vaccines stop the spread of the infection.
10. Immune protection only comes from a vaccine.
None of us are so naïve as to expect a direct apology from critics at my employer, Stanford University, or in government, academic public health, and the media. But to ensure that this never happens again, government leaders, power-driven officials, and influential academics and advisors often harboring conflicts of interest must be held accountable. Personally, I remain highly skeptical that any government investigation or commission can avoid politicization. Regardless of their intention, all such government-run inquiries will at least be perceived as politically motivated and their conclusions will be rejected outright by many. Those investigations must proceed, though, if only to seek the truth, to teach our children that truth matters, and to remember G.K. Chesterton's critical lesson that "Right is right, even if nobody does it. Wrong is wrong, even if everybody is wrong about it."
The last three and a half years have been times of enormous upheaval. It has affected politics, economics, culture, media, and technology. It’s not just about the spreading of economic, cultural, and demographic decay. Millions and billions of lives have been wrecked, to be sure, but there is also a big impact on the way we see the world around us.
What we once trusted, we now doubt and even disbelieve as a matter of new habit. The simple categories of understanding that we once deployed to make sense of the world have been tested, challenged, and even overthrown. Old forms of ideological commitments have opened their way to new. This particularly pertains to intellectuals.
Or should in any case. If you have not shifted your thinking in some respect over these years, you are either a prophet, asleep, or in denial. The way social media works today, influencers are reluctant to admit it lest risk their followings built out of a prior cultural landscape. This is really too bad. There is nothing wrong with changing, adapting, migrating, and calling out truth even if that contradicts what you once said or how you used to believe.
There is no need to change your principles or ideals. What should change in light of evidence is your evaluation of the problems and threats, your outlook on the relative priorities of focus, your perceptions of the functionality of institutional structures, your awareness of issues and concerns about which you had limited prior knowledge, your political and cultural allegiances, and so on.
These days, this intellectual migration seems mainly to have affected the left. Nearly daily I find myself having the same conversations with people in person, on the phone, or online. It is from an Obama voter and someone with traditionally “liberal” allegiances.
The Covid era utterly shocked them in what they discovered about their own tribe. They aren’t liberal at all. They supported universal quarantine, forced face coverings, and then mandatory jabs pushed by a tax-funded corporate monopoly. Concerns about human rights, civil liberties, and the common good suddenly evaporated. Then of course they turned to the most blunt instrument of all: censorship.
The trauma felt by principled people who imagined themselves to be “on the left” is palpable. But the same is true of people “on the right” who were aghast to observe that it was Trump and his administration that greenlighted lockdowns, spent many trillions forcing Covid compliance, and then threw public monies at Big Pharma to rush a shot by bypassing all standards of necessity, safety, and effectiveness.
The promise to “make America great again” ended in wreckage coast-to-coast. For Trump partisans, this realization that it all happened under their hero is hard to take, a triangulating rope-a-dope. Even more strangely, it was the “never Trumpers” on the right who most strongly supported lockdowns, masking, and shot mandates.
The libertarians are another story entirely, one that nearly surpasses understanding. Among the higher echelons of this faction in academia and think tanks, the silence from the start and even years later was truly deafening. Instead of standing up to totalitarianism, as the whole of the intellectual tradition had prepared them to do, they deployed their clever heuristics to justify outrages against core freedoms, even the freedom to associate.
So, yes, observing one’s own tribe collapse into craven careerism and coercion is disorienting. But the problem goes even deeper. The most striking alliance of our time has been to observe the lockstep of the elites in government, media, tech, and academia. The reality blows apart the traditional binary of public vs private that has dominated ideological discussion for centuries.
I used to regard the government as extremely inept/incompetent, fairly corrupt, and facing incentives that pushed agencies/officials to be generally inept & corrupt.
Now, I regard the government as fundamentally evil on par with any other classical murderous sociopathic regime -- something that the pandemic exposed. (To be absolutely clear, this is not a Nazi comparison, they were far beyond a 'classical' evil murderous regime.)
1. The US government went out of their way to suppress, sabotage, and destroy every effective covid treatment, which by itself caused hundreds of thousands of deaths if not millions around the world (the US agencies are extremely influential for the rest of the world). Unfortunately, there were a few prominent doctors who were actively complicit in this, including one who lied under oath in an affidavit submitted on behalf of his hospital in a lawsuit brought by a covid patient’s family to allow them to give Ivermectin to the patient. Among other things, this doctor claimed that there had been NO clinically discernible improvement after the first round of Ivermectin was administered to the patient, which was patently false as was described in an affidavit by an outside physician who *detailed the specific clinical improvements that were documented in the patient’s medical records from that hospital*. I personally know the physician who wrote this affidavit & can attest that he is not a liar. The patient ultimately died amidst the court wrangling.
brownstone.org [2023-08-21] Jeffrey A. Tucker, August 12, 2023 link archive General
Comparison to Smallpox Outbreaks in the Mid 1800's
Initially Jenner’s claims (first published in 1798) were met with much skepticism, as many physicians had observed patients develop cowpox and subsequently smallpox, and others questioned the basic validity of his studies (one physician who tested 3 children with Jenner’s vaccine found all 3 subsequently developed smallpox after inoculation, with similar results obtained by other physicians). Nonetheless, the practice gradually caught on, became a larger share of physician income, became more and more popular within the medical field, and over the next hundred years, the number of dissenting physicians gradually diminished. However, what is relatively unknown now is that many did speak out, and published literature with data showing serious issues with the vaccine.
[...]
Mandatory Smallpox Vaccination
As it became clear that the smallpox vaccine was unable to prevent disease as initially promised, the medical profession moved the goal posts from lifelong “perfect” immunity to “milder disease” to justify vaccination, a tactic that has since repeated with other vaccination campaigns.
Mr. Henry May, writing to the Birmingham Medical Review, in January, 1874 reported that deaths as a result of vaccination were often not reported because of an allegiance to the practice. Often a vaccinated person was recorded as having died from another condition such as chicken pox or erroneously listed as unvaccinated.
This corruption of the vital statistics creates many challenges in assessing the efficacy of immunization, and is also why many authors argue no metric can be used to assess COVID-19 immunizations except total number of deaths (independent of cause) as this cannot be fudged. Of note, a different significant overlap exists with the early Polio campaigns (also detailed within the book), where “Polio” diagnostic criteria was repeatedly adjusted to meet the political need for Polio cases.
Governments responded to this skepticism by progressively using more and more force to mandate vaccination. Vaccination was made compulsory in England in 1853, with stricter laws passed in 1867. In the United States, Massachusetts created a set of comprehensive vaccination laws in 1855 (which created the Supreme Court case Jacobson v. Massachusetts a case that is frequently cited about state enforced vaccination). Lemuel Shattuck emphasized the need for vaccination and pushed for house-to-house vaccination to be enforced by the authority of the City of Boston in an 1856 report, also noting ““The City has already provided that no unvaccinated child shall be admitted into the public schools.”
[...]
A situation emerged I term the vaccine positive feedback cycle. Keep in mind that most systems in nature are instead negative feedback systems. In these, when something occurs, it self-corrects the system and turns it off rather than accelerating it, as occurs in a positive feedback system.
The cycle is as follows:
A concerning disease exists
↓
Immunization is cited as a potential solution to the problem
↓
A preliminary immunization campaign is conducted and makes the problem worse
↓
As the problem is now worse, the need for immunizations to address it increases and another campaign is conducted
↓
This makes the problem worse
↓
This increases the need for more aggressive measures to increase immunization
↓
This makes the problem worse and further perpetuates the cycle, before long leading to very questionable governmental policies designed to force unwilling parties to vaccinate.
The underlying drivers of this process seem to be an unquestionable faith in vaccination, a conviction dating back to the days of smallpox, that vaccinating an ever increasing proportion of the population through vaccination can end epidemics (now termed herd immunity), and the government having limited options to address the issue besides immunizations and governmental force.
[...]
Effects of Mandatory Smallpox Vaccination
In accordance the positive feedback cycle, these results were found everywhere. Within the United States, as smallpox worsened in Boston, in 1855, the government enacted strict enforcement of vaccination. It was followed by the epidemics of 1859-1860, 1864-1865, 1867 (these were all similar in size to earlier epidemics), and then infamous 1872-1873 epidemic which dwarfed all previous epidemics (proving fatal to 1040 persons, at a rate of 280 deaths per 100,000 people).
By the end of 1868, more than 95 percent of the inhabitants of Chicago had been vaccinated. After the Great Fire of 1871 (it leveled the city), strict vaccine laws were passed, and vaccination was made a condition of receiving relief supplies. Chicago was then hit with a devastating smallpox epidemic in 1872 where over 2000 persons contracted smallpox, with over 25% dying, and the fatality rate among children under 5 being the highest ever recorded.
“The global reset is not a “response” to the process of collapse we are trapped in today. No, the global reset as implemented by central banks and the BIS/IMF is the cause of the collapse. The collapse is a tool, a flamethrower burning a great hole in the forest to make way for the foundations of the globalist Ziggurat to be built....economic disaster serves the interests of elitists.”
Now in 2020 we see the globalist plan coming to fruition, with the elites revealing what appears to be their intent to launch their reset in 2021. The World Economic Forum officially announced the Great Reset initiative as part of their Covid Action Platform last week, and a summit is scheduled in January 2021 to discuss their plans more openly with the world and the mainstream media.
[...]
The new world order, the global reset, is a long running scheme to centralize power, but in a way that is meant to be sustained for centuries to come. The elites know that it is not enough to achieve global governance by force alone; such an attempt would only lead to resistance and eternal rebellion. No, what the elites want is for the public to ASK, even beg for global governance. If the public is tricked into demanding it as a way to save them from the horrors of global chaos, then they are far less likely to rebel against it later. Problem – reaction – solution.
alt-market.com [2020-06-28] Brandon Smith, 18 June 2020 link archive General
Joining me today is Professor Richard Werner, here to discuss COVID-19 from an economic perspective, and the role central banks are playing in this rapidly shifting financial and societal landscape.
Note: At 57:55 Werner talks about his involvement with the World Economic Forum's Global Leaders of Tomorrow, meeting Klaus Schwab, and apparent push-back when asking critical questions.
bitchute.com [2022-02-24] The Last American Vagabond channel, August 15th, 2021 link archive General
This video documents the earnings of prominent billionaires since march, the departure of major CEOs over the last year, and asks questions about the future.
The 2021 pandemic documentary Plant Lockdown produced by award winning film-maker James Patrick garnered tens of millions of views before it was expunged from virtually every platform on earth.
Listen to his question about “therapeutic nihilism” and then a follow-on about the Emergency Use Authorization mechanism as the excuse for the suppression of early therapeutics. Because it was worldwide, the American EUA could not have been the reason why sick patients were denied life-saving medications all over the globe.
rumble.com [2021-02-10] planetlockdown on Rumble, January 19, 2021 link archive General
UNITED NATIONS (Reuters) - Hundreds of thousands of children could die this year due to the global economic downturn sparked by the coronavirus pandemic and tens of millions more could fall into extreme poverty as a result of the crisis, the United Nations warned on Thursday.
reuters.com [2021-03-02] By Michelle Nichols, APRIL 17, 2020 link archive General
Almost half the global workforce – 1.6 billion people – are in “immediate danger of having their livelihoods destroyed” by the economic impact of Covid-19, the International Labour Organization has warned.
theguardian.com [2021-03-02] Phillip Inman, April 29, 2020 link archive General
The World Bank bonds offer investors high interest payments in return for taking on the risk of losing a certain amount or all of their money if pandemics occur. That includes the current coronavirus pandemic.
But prices of those bonds have plunged, as investors flee with the number of cases surging.
According to ratings agency DBRS Morningstar, investors who hold the riskier of the two bonds could be losing their entire principal amount soon, with the firm saying that the price should have dropped more than 80%.
cnbc.com [2021-05-29] Weizhen Tan, MAR 17 2020 link archive General
GDP levels had already recovered to pre-pandemic levels when coercive vaccine mandates were introduced
The government measures in response to the declaration of the pandemic caused a drop in the level of economic activity as measured by the GDP (gross domestic product). By drawing trendlines over the GDP data we can estimate what the economic levels would have been without the government covid-19 measures. Conceptually it looks like the following chart.
[...]
freedomandinvesting.substack.com [2024-01-22] Lex Acker, January 21, 2024 link archive General
As ordinary people around the world suffer from the health and economic impacts of the pandemic, billionaires have actually seen their fortunes expand. According to Institute for Policy Studies analysis of Forbes data, the combined wealth of all U.S. billionaires increased by $2.071 trillion (70.3 percent) between March 18, 2020 and Ocobter 15, 2021, from approximately $2.947 trillion to $5.019 trillion. Of the more than 700 U.S. billionaires, the richest five (Jeff Bezos, Bill Gates, Mark Zuckerberg, Larry Page, and Elon Musk) saw an 123 percent increase in their combined wealth during this period, from $349 billion to $779 billion. We will be regularly updating this analysis here.
[...]
inequality.org [2023-03-27] December 21, 2022 link archive General
COVID-19 is dramatically changing the economic landscape. Some industries are faring well while others are being devastated by the pandemic. Businesses are rapidly adapting to the demands and peculiarities of living within the constraints of a pandemic. Of particular concern to me is the plight of small businesses. In many ways, small businesses are the lifeblood of the American economy. Indeed, before COVID-19, various studies found that small businesses accounted for about 50% of private-sector jobs. Moreover, Americans highly value their right to start a small business – be it a local restaurant, a small retail shop, or an online business.
But small businesses historically have been adversely impacted by recessions in part because many small businesses operate on limited cash flow. This begs the question: how are small businesses enduring this now prolonged impact of COVID-19?
When COVID-19 began in the spring and many states shut down or substantially reduced various business services, it was clear that small businesses were skeptical they could survive a prolonged pandemic. For example, in an April 2020 survey of 5,850 small businesses across the country, Main Street America found that 75% of respondents reported that their business revenues had declined by more than half. And 66% of respondents predicted their business would be at risk of closing if the economic impact of the pandemic continued for 3 to 5 months.
[...]
Moreover, certain industries and certain types of small businesses have been particularly hard hit by the pandemic. Studies have found that small businesses in certain geographic areas have been strongly hit by the economic impact of the pandemic, including those in more densely populated cities. And most studies have found that minority-owned small businesses have been particularly hard hit by COVID-19. In addition, studies estimate that many of the hardest-hit industries will not likely return to the levels of business that existed pre-COVID-19 for at least 5 years. This includes industries which involve a lot of small businesses such as restaurants, hospitality, retail and education. Finally, new business start-ups have also fallen dramatically since the spring – a trend that needs to substantially change for our economy to recover from this pandemic!
Despite all these challenges, it appears that small businesses are rapidly adapting to the new normal of running a business amidst a pandemic. Locally-owned restaurants have added curbside pickup and are gradually expanding the to-go portion of their business. Local retailers are also now frequently offering curbside pickup in addition to adjusting their hours, limiting the number of customers, and even offering special hours for their most vulnerable customers. Various small businesses are substantially expanding their online offerings. Small business manufacturers are adjusting their work environments to allow for appropriate social distancing through the creation of manufacturingpods. Small businesses generally are greatly expanding their work-at-home options and related support capabilities. And at least some new small business opportunities are being created amidst this pandemic – note the advent of COVID-19 disinfection services!
[...]
infotechconsulting.com [2022-05-30] Rob Kneuper, Aug 17, 2020 link archive General
Market-driven economies, privatization, and the medicalization of health, amongst other factors, have all been shaped by, and are shaping corporate behaviors. This sits alongside the rapid growth in size and internationalisation of the very largest corporations, with the revenues of companies like Walmart, Volkswagen and Amazon now exceeding that of entire countries. The 'industrial epidemic' hits vulnerable populations the hardest and is a direct consequence of corporate practices. These practices include the production and sale of unhealthy commodities, tax evasion, child labor, marketing to children, the distortion of science, and lobbying. Collectively, they have been described as 'commercial determinants of health'. The current COVID-19 pandemic has seen many larger corporations increase their revenues, while they have also been responsible for growing inequities and negative impacts on population and planetary health. The social and economic impacts of the COVID-19 pandemic are vast, yet little is known about corporate political practices and the action of corporate power during the pandemic, and how these are shaping population and planetary health. There is evidence that alcohol and tobacco companies lobbied for carcinogenic products to be listed as essential commodities during the first lockdown period. Tobacco companies have used the pandemic to polish their bad reputation, by investing in vaccines development and in community responses. Food companies have used the pandemic to put a health halo on ultra-processed food products. Some have called this `disaster capitalism', where corporations use crises to strengthen their market position and social power. For this Research Topic, we are interested in exploring the impacts of corporate power and political practices in response to the COVID-19 pandemic on public and planetary health. We have no restriction on the type of industry that is discussed. Manuscripts must provide scientific knowledge and evidence relevant to public health policy, research or/and practice. We are interested in receiving Original Research articles, Systematic Reviews, Reviews, Policy and Practice Reviews, and Community Case Studies. Submissions could cover but are not limited to the following topics: § Corporate structural, instrumental and discursive power and the COVID-19 pandemic, in relation to public and/or planetary health § Corporate political practices and their impacts on public and/or planetary health during the COVID-19 pandemic, including the influence on science, policy and practice; § Ethical issues in public health related to corporations and their responses to the COVID-19 pandemic; Conflicts of interest in public health during the COVID-19 pandemic. Special note: We will not accept manuscripts reporting on research that is funded by the tobacco, alcohol, food, gambling, arm, oil, pharmaceutical, and other health-harming industries and third parties affiliated with them, or from authors who have previously worked for or with them. All authors are asked to declare their current or previous interactions with these industries when they exist, and any interaction they had with any other industry(ies) described in their manuscript. We will reject manuscripts where there are clear conflicts of interest.
The Federal Reserve has moved with unprecedented force and speed to pump huge amounts of cash into the financial system to ease disruptions that have escalated since the viral outbreak
WASHINGTON -- The Federal Reserve moved with unprecedented force and speed Friday to pump huge amounts of cash into the financial system to ease disruptions that have escalated since the viral outbreak.
The New York Federal Reserve Bank said it will offer $1 trillion of overnight loans a day through the end of this month to large banks. That is in addition to $1 trillion in 14-day loans it is offering every week. Banks, so far, have not borrowed nearly as much as the New York Fed is offering, and the loans are quickly repaid. None of the funding is from taxpayer dollars. Wall Street analysts say the huge number is intended to calm markets by demonstrating that the Fed's ability to lend short-term is nearly unlimited.
The Fed is also buying Treasury bonds at a furious pace, and will soon run through the $500 billion in purchases it announced on Sunday. It is also accelerating its purchases of mortgage-backed securities. Most analysts expect they will buy more.
“The Fed has just worked with unprecedented speed,” said Steven Friedman, a former economist at the New York Fed and senior macroeconomist at MacKay Shields, an asset manager. "I think there will be no hesitation on their part about buying as many Treasuries and mortgage-backed securities as necessary."
All the Fed's emergency steps are intended to pump cash into a financial system that has seen a spike in demand for dollars as investors unload Treasuries, municipal bonds, and other securities. With the economy likely in recession, banks, money market funds and other institutional investors are increasingly wary about holding securities that may lose value.
[...]
abcnews.go.com [2022-06-30] Christopher Rugaber, March 21, 2020 link archive General
WASHINGTON (AP) — The Federal Reserve moved with unprecedented force and speed Friday to pump huge amounts of cash into the financial system to ease disruptions that have escalated since the viral outbreak.
The New York Federal Reserve Bank said it will offer $1 trillion of overnight loans a day through the end of this month to large banks. That is in addition to $1 trillion in 14-day loans it is offering every week. Banks, so far, have not borrowed nearly as much as the New York Fed is offering, and the loans are quickly repaid. None of the funding is from taxpayer dollars. Wall Street analysts say the huge number is intended to calm markets by demonstrating that the Fed’s ability to lend short-term is nearly unlimited.
The Fed is also buying Treasury bonds at a furious pace, and will soon run through the $500 billion in purchases it announced on Sunday. It is also accelerating its purchases of mortgage-backed securities. Most analysts expect they will buy more.
“The Fed has just worked with unprecedented speed,” said Steven Friedman, a former economist at the New York Fed and senior macroeconomist at MacKay Shields, an asset manager. “I think there will be no hesitation on their part about buying as many Treasuries and mortgage-backed securities as necessary.”
All the Fed’s emergency steps are intended to pump cash into a financial system that has seen a spike in demand for dollars as investors unload Treasuries, municipal bonds, and other securities. With the economy likely in recession, banks, money market funds and other institutional investors are increasingly wary about holding securities that may lose value.
Companies will see revenue and earnings plunge, while local and state governments are likely to see lower tax revenue. That makes it harder for them to borrow.
“There is a growing certainty that we’re facing an economic contraction, so it’s natural for investors to become more concerned about risk,” Friedman said. “The Fed is trying to play the role of shock absorber.”
Topline: As stocks headed for their worst day since 1987’s Black Monday Crash, the Federal Reserve announced further measures to prop up liquidity including a potential injection of more than $1.5 trillion into the market; stocks responded immediately, cutting losses in half on the announcement, before dropping back down 8%.
The Fed said it will ramp up its overnight funding operations—buying “repos,” or repurchase agreements—by $1.5 trillion over the next two days.
“These changes are being made to address highly unusual disruptions in Treasury financing markets associated with the coronavirus outbreak,” the New York Fed said in a statement on Thursday afternoon.
The Fed also widened the range for its reserve management purchases—which had previously been restricted to short-term Treasury bills—to include other types of financial instruments.
The moves are designed to preserve liquidity in the market; in other words, the Fed wants to prevent “freezes” and make sure buyers and sellers still have the ability to trade.
It’s the third time in four days the New York Fed has announced that it will bulk up lending in the repo market: on Tuesday, it announced an injection of $50 billion, and it added another $25 billion on Wednesday.
Stocks initially pared back nearly half their losses on the announcement, but within the hour had dropped back close to their previous daily lows; at 2:00 p.m. EST on Thursday, the Dow Jones Industrial Average was down 8%.
Key background: Stocks rallied on Tuesday this week after President Trump promised to introduce an economic stimulus package to address the crisis, then dropped again on Wednesday when details about that plan were slow to emerge. European stocks cratered on Thursday morning after President Trump announced that he would ban travel to the U.S. from Europe for 30 days. The Fed’s actions this week have been focused on the repo market, where it lends financial institutions short term money overnight so they have enough cash to cover their operations throughout the day. Repo is short for “repurchase agreement"; in these transactions, the Fed buys securities from a seller (a bank, or hedge fund, for example) who agrees to repurchase them later on with a bit of interest. This helps the Fed inject more cash into the banking system.
[...]
forbes.com [2022-06-30] Sarah Hansen, Mar 12, 2020 link archive General
Covid-19 has killed more than one million people in the U.S., a toll mounting by some 350 people a day. A range of other chronic diseases and acute threats to health also worsened during the pandemic, data show, as people missed screenings, abandoned routines and experienced loss and isolation.
[...]
brighteon.com [2022-08-01] Brianna Abbott, July 31, 2022 link archive General
Question What is the period prevalence and incidence of SARS-CoV-2 infection among people experiencing homelessness in Toronto, Canada?
Findings In this prospective cohort study of 736 people experiencing homelessness in Toronto, 30% of individuals had a history of infection by summer 2021 and a further 30% experienced incident infection within 6 months. Incident infection was significantly associated with reporting after the SARS-CoV-2 Omicron variant became dominant, recent immigration to Canada, and recent alcohol consumption.
Meaning In this study, people experiencing homelessness in Toronto had high SARS-CoV-2 incident infection rates.
Abstract
Importance People experiencing homelessness are at high risk of SARS-CoV-2 infection. Incident infection rates have yet to be established in these communities and are needed to inform infection prevention guidance and related interventions.
Objective To quantify the SARS-CoV-2 incident infection rate among people experiencing homelessness in Toronto, Canada, in 2021 and 2022 and to assess factors associated with incident infection.
Design, Setting, and Participants This prospective cohort study was conducted among individuals aged 16 years and older who were randomly selected between June and September 2021 from 61 homeless shelters, temporary distancing hotels, and encampments in Toronto, Canada.
Exposures Self-reported housing characteristics, such as number sharing living space.
Main Outcomes and Measures Prevalence of prior SARS-CoV-2 infection in summer 2021, defined as self-reported or polymerase chain reaction (PCR)– or serology-confirmed evidence of infection at or before the baseline interview, and SARS-CoV-2 incident infection, defined as self-reported or PCR- or serology-confirmed infection among participants without history of infection at baseline. Factors associated with infection were assessed using modified Poisson regression with generalized estimating equations.
Results The 736 participants (415 of whom did not have SARS-CoV-2 infection at baseline and were included in the primary analysis) had a mean (SD) age of 46.1 (14.6) years; 486 (66.0%) self-identified as male. Of these, 224 (30.4% [95% CI, 27.4%-34.0%]) had a history of SARS-CoV-2 infection by summer 2021. Of the remaining 415 participants with follow-up, 124 experienced infection within 6 months, representing an incident infection rate of 29.9% (95% CI, 25.7%-34.4%), or 5.8% (95% CI, 4.8%-6.8%) per person-month. Report after onset of the SARS-CoV-2 Omicron variant was associated with incident infection, with an adjusted rate ratio (aRR) of 6.28 (95% CI, 3.94-9.99). Other factors associated with incident infection included recent immigration to Canada (aRR, 2.74 [95% CI, 1.64-4.58]) and alcohol consumption over the past interval (aRR, 1.67 [95% CI, 1.12-2.48]). Self-reported housing characteristics were not significantly associated with incident infection.
Conclusions and Relevance In this longitudinal study of people experiencing homelessness in Toronto, SARS-CoV-2 incident infection rates were high in 2021 and 2022, particularly once the Omicron variant became dominant in the region. Increased focus on homelessness prevention is needed to more effectively and equitably protect these communities.
New data show that Covid-19 is far worse for children than seasonal influenza, as long suspected.
[...]
[NOTE: In response to questions from readers and colleagues, I've edited the following paragraph. For transparency, you can see the changes below in bold. For a more complete follow up Inside Medicine on this and related issues, click here.]
Covid-19 killed (i.e., appeared on death certificates as either an underlying or contributing cause) 596 (around 600) children in 2021, which is far more than influenza ever kills in any given year. At the peak of Omicron, 158 (156; two more dead children have been added to the dataset) US children died of Covid-19 in a single month (January 2022). In the 10 years leading up to the Covid-19 pandemic, an average of 150(120) children died of flu per year—and that was without masking or distancing.
These irrefutable figures, reported by the Centers for Disease Control and Prevention, reveal that last year, pediatric Covid-19 deaths were around 490% (500%) that of pediatric flu deaths in a typical 21st century season.
Make no mistake: Covid-19 is imparting an unusual burden on children compared to all other respiratory viruses. Since the turn of the century, there have been just 7 instances in which a respiratory virus killed (i.e., appeared on death certificates as an underlying or contributing cause) more than 65 children in a single month in the US. Influenza did it twice: once during the H1N1 pandemic of 2009 (which hit children harder than most realize) and once in March of 2003 (2009; typo). Covid-19 accounts for each of the other 5 instances, all of which occurred between just August 2021 and February (January; typo) 2022. In fact, of known respiratory viruses, only Covid-19 has ever killed more than 100 US children in a month (underlying cause) in the modern era (for as far back as I can track into the 1990s); it also did so as an underlying or contributing cause) three times during Delta and Omicron alone. Flu did that once (underlying or contributing cause), during the peak of the 2009-2010 H1N1 pandemic.
Yes, this reflects more contagious variants. Yes, this reflects decreased adherence to physical distancing as the pandemic has dragged on. That’s the point.
Covid-19 killed more than 100 US children in August 2021, September 2021, and January 2022. No other virus has done that in the modern era, including pandemic H1N1 (2009).
Hint: It's a mild flu year so far, yet there are more flu than COVID hospitalizations in the UK.
[...]
Below is a CDC chart that compares the % of doctor visits that are for respiratory infections by week. Each color represents a different year. This year is black. Infections peaked early and are already falling. Another flu may appear later in the season; this happens sometime. But you can see we are in the normal ballpark. https://www.cdc.gov/flu/weekly/index.htm
Question Are hospital outcomes of SARS-CoV-2 variant B1.1.529 (SARS-CoV-2 Omicron variant) comparable with outcomes of seasonal influenza infections among hospitalized patients?
Findings In this cohort study of 5212 patients hospitalized with the SARS-CoV-2 Omicron variant or influenza A or B in Switzerland, the SARS-CoV-2 Omicron variant was associated with an approximately 1.5-fold higher risk of in-hospital all-cause mortality up to day 30 compared with influenza.
Meaning These findings suggest that, despite virus evolution and improved management strategies, patients with the SARS-CoV-2 Omicron variant had a higher risk of in-hospital mortality than those with influenza.
Abstract
Importance With the ongoing COVID-19 pandemic, it is crucial to assess the current burden of disease of community-acquired SARS-CoV-2 Omicron variant in hospitalized patients to tailor appropriate public health policies. Comparisons with better-known seasonal influenza infections may facilitate such decisions.
Objective To compare the in-hospital outcomes of patients hospitalized with the SARS-CoV-2 Omicron variant with patients with influenza.
Design, Setting, and Participants This cohort study was based on a national COVID-19 and influenza registry. Hospitalized patients aged 18 years and older with community-acquired SARS-CoV-2 Omicron variant infection who were admitted between January 15 and March 15, 2022 (when B.1.1.529 Omicron predominance was >95%), and hospitalized patients with influenza A or B infection from January 1, 2018, to March 15, 2022, where included. Patients without a study outcome by August 30, 2022, were censored. The study was conducted at 15 hospitals in Switzerland.
Exposures Community-acquired SARS-CoV-2 Omicron variant vs community-acquired seasonal influenza A or B.
Main Outcomes and Measures Primary and secondary outcomes were defined as in-hospital mortality and admission to the intensive care unit (ICU) for patients with the SARS-CoV-2 Omicron variant or influenza. Cox regression (cause-specific and Fine-Gray subdistribution hazard models) was used to account for time-dependency and competing events, with inverse probability weighting to adjust for confounders with right-censoring at day 30.
Results Of 5212 patients included from 15 hospitals, 3066 (58.8%) had SARS-CoV-2 Omicron variant infection in 14 centers and 2146 patients (41.2%) had influenza A or B in 14 centers. Of patients with the SARS-CoV-2 Omicron variant, 1485 (48.4%) were female, while 1113 patients with influenza (51.9%) were female (P = .02). Patients with the SARS-CoV-2 Omicron variant were younger (median [IQR] age, 71 [53-82] years) than those with influenza (median [IQR] age, 74 [59-83] years; P < .001). Overall, 214 patients with the SARS-CoV-2 Omicron variant (7.0%) died during hospitalization vs 95 patients with influenza (4.4%; P < .001). The final adjusted subdistribution hazard ratio (sdHR) for in-hospital death for SARS-CoV-2 Omicron variant vs influenza was 1.54 (95% CI, 1.18-2.01; P = .002). Overall, 250 patients with the SARS-CoV-2 Omicron variant (8.6%) vs 169 patients with influenza (8.3%) were admitted to the ICU (P = .79). After adjustment, the SARS-CoV-2 Omicron variant was not significantly associated with increased ICU admission vs influenza (sdHR, 1.08; 95% CI, 0.88-1.32; P = .50).
Conclusions and Relevance The data from this prospective, multicenter cohort study suggest a significantly increased risk of in-hospital mortality for patients with the SARS-CoV-2 Omicron variant vs those with influenza, while ICU admission rates were similar.
Clinical concerns over both COVID-19 and influenza should have remained on the vulnerable elderly population, particularly those in senior centers. Instead we have seen a two-year media blitz on vaccinating young healthy working age persons and children. Portmann and colleagues published a sobering report on hospitalized cases of Omicron and Influenza A/B infections in Switzerland. The in-hospital mortality rates were 7.0 and 4.4% with 8.5 and 15.3% incurring cardiovascular events in the SARS-CoV-2 and Influenza A/B groups, respectively. This translated into nearly identical outcomes (ICU admission and death) at 30 days in both groups. There appeared to be no impact of antecedent vaccination for either disease but for different reasons. The COVID-19 vaccinations failed to stop hospitalization with the majority having been immunized. There was no statistical difference in death among those vaccinated verses not, 7.2 vs 9.3%, p=0.05, respectively. Influenza vaccination appeared to have no impact because of very poor utilization (10%) with considerable missing data.
jamanetwork.com [2023-02-17] Lea Portmann, Marlieke E. A. de Kraker, Georg Fröhlich, ..., Rami Sommerstein, February 15, 2023 link archive General
New guidelines from the CDC Friday bring Covid precautions in line with those of other respiratory viruses
A case of Covid no longer means isolating for five days, according to the latest guidance from the Centers for Disease Control and Prevention released Friday. It’s the latest sign of the virus’s normalization four years after it upended our lives.
You should now follow the same precautions with Covid as you take with the flu, according to new guidelines from the CDC. That means staying home until you’ve gone a day with no fever and symptoms start to improve. Take other precautions for the next five days, including wearing a mask and limiting close contact with others.
? More good news! I enjoyed a hearty laugh this morning reading the Wall Street Journal’s sidesplitting story headlined, “It’s Official: We Can Pretty Much Treat Covid Like the Flu Now. Here’s a Guide.” The sub-headline farcically explained, “New guidelines from the CDC Friday bring Covid precautions in line with those of other respiratory viruses.” Now that’s entertainment. That is value for money.
Why now? It’s election season! And Glorious Leader Biden needs a win. So yesterday’s misinformation that used to get you banned off social media and slapped on a Homeland Security list somewhere is now the CDC’s official guidance. Biden beat a virus.
Ah, the good old days. Back when C&C was just musings on Facebook, I assiduously avoided directly saying covid was like the flu. The censors and I played cat and mouse for months, while I used the word “So” to fill in the obvious blank. Eventually they caught on, and after two 7-day bans and then a 30-day account lockdown, C&C moved out of Meta.
But now the CDC says trust them, covid was a civilization-destroying virus for a few months. It totally justified the economy-destroying lockdowns and Constitution-shredding mandates. But now it’s just a seasonal flu! Don’t worry! Get extra fluids and rest at home! Never mind!
Science. Shut up!
But the lingering question remains: are hardcore zero-covid fanatics still screeching that covid is ten times worse than ebola … spreading misinformation? I mean, if the CDC is the gold standard, what about them?
How times change.
wsj.com [2024-03-03] Sumathi Reddy, March 1, 2024 link archive General
The BIden Administration continues to double and even triple down on the lie that the Covid Vaccines are safe and effective after the vaccines have caused countless deaths and injuries reported worldwide. On top of that glaring omission is the sudden disappearance of the 40 million seasonal flu cases that essentially vanished. While Biden officials admitted to counting any and everything as a Covid death in order to market the Covid Vaccines.
banned.video [2023-01-05] Bowne Report, Dec 19, 2022 link archive General
BACKGROUND. Despite guidelines promoting the prevention and aggressive treatment of ventilator-associated pneumonia (VAP), the importance of VAP as a driver of outcomes in mechanically ventilated patients, including patients with severe COVID-19, remains unclear. We aimed to determine the contribution of unsuccessful treatment of VAP to mortality in patients with severe pneumonia.
METHODS. We performed a single-center prospective cohort study of 585 mechanically ventilated patients with severe pneumonia and respiratory failure, 190 of whom had COVID-19, who underwent at least one bronchoalveolar lavage. A panel of ICU physicians adjudicated pneumonia episodes and endpoints based on clinical and microbiologic data. Given the relatively long ICU length of stay among patients with COVID-19, we developed a machine learning approach called CarpeDiem, which groups similar ICU patient-days into clinical states based on electronic health record data.
RESULTS.CarpeDiem revealed that the long ICU length of stay among patients with COVID-19 is attributable to long stays in clinical states characterized primarily by respiratory failure. While VAP was not associated with mortality overall, mortality was higher in patients with one episode of unsuccessfully treated VAP compared with successfully treated VAP (76.4% versus 17.6%, P < 0.001). In all patients, including those with COVID-19, CarpeDiem demonstrated that unresolving VAP was associated with transitions to clinical states associated with higher mortality.
CONCLUSIONS. Unsuccessful treatment of VAP is associated with greater mortality. The relatively long length of stay among patients with COVID-19 is primarily due to prolonged respiratory failure, placing them at higher risk of VAP.
Unsurprisingly, the study found that people with bacterial pneumonia who were on ventilators had the highest mortality. Although their analysis restricted consideration to bacterial pneumonia cases detected 48 hours after ventilation, they did not distinguish between undiagnosed cases of bacterial pneumonia upon admission and those acquired in-hospital (nosocomial infection). The rate of co-infection is not clear either, due to insufficient testing for bacterial pneumonia in patients once diagnosed with COVID-19.
The study leads to the stunning potential that perhaps 58% of “COVID” cases were respiratory issues other than COVID (43% bacterial pneumonia, 16% non-pathogen causes of respiratory failure). Treated as “COVID”, these patients were doomed to a fate of non-treatment due to mis- or under-diagnosis.
jci.org [2023-05-23] Catherine A. Gao, Nikolay S. Markov, ..., Benjamin D. Singer, April 27, 2023 link archive General
Unpacking The "Science" Behind the Annual Vaccination Scam
Story at a Glance:
• A huge business exists that revolves around making people afraid of the seasonal flu so vaccines can be sold each year.
• Many of the fundamental ideas supporting this practice are erroneous or rest on a very shaky foundation—for example, no one actually knows how dangerous the flu is and flu shots have been shown to make you more likely to become ill from the flu.
• Much of the COVID-19 playbook was copied from the one developed to sell flu shots. For this reason, understanding the malfeasance with the influenza vaccination program provides a valuable context for understanding what is happening right now and why treatments for these conditions are never allowed to see the light of day.
Recently, I was consulted by a public figure to answer a seemingly simple question—is COVID-19 less deadly than the flu now?
Unfortunately, this is actually a very difficult question to answer, to the point I would have never imagined how difficult it was had I not looked into it myself. After I reviewed the data with the public figure, I realized that there is a lot of value in exploring that answer with each of you as it cuts to the heart of the pandemic industrial complex.
[...]
midwesterndoctor.com [2023-10-06] A Midwestern Doctor, October 5, 2023 link archive General
Once a punishable offense by the online censors, the CDC is now telling people to treat COVID just like the flu. Meanwhile, a 9th booster has been added with the 10th on the way.
Welcome to New World Next Week – the video series from Corbett Report and Media Monarchy that covers some of the most important developments in open source intelligence news. This week:
Since the beginning of the COVID-19 pandemic, reduced incidence of many viral and bacterial infections has been reported in children: bronchiolitis, varicella, measles, pertussis, pneumococcal and meningococcal invasive diseases. The purpose of this opinion paper is to discuss various situations that could lead to larger epidemics when the non-pharmaceutical interventions (NPI) imposed by the SARS-CoV-2 epidemic will no longer be necessary. While NPIs limited the transmission of SARS-CoV-2, they also reduced the spread of other pathogens during and after lockdown periods, despite the re-opening of schools since June 2020 in France. This positive collateral effect in the short term is welcome as it prevents additional overload of the healthcare system. The lack of immune stimulation due to the reduced circulation of microbial agents and to the related reduced vaccine uptake induced an "immunity debt" which could have negative consequences when the pandemic is under control and NPIs are lifted. The longer these periods of "viral or bacterial low-exposure" are, the greater the likelihood of future epidemics. This is due to a growing proportion of "susceptible" people and a declined herd immunity in the population. The observed delay in vaccination program without effective catch-up and the decrease in viral and bacterial exposures lead to a rebound risk of vaccine-preventable diseases. With a vaccination schedule that does not include vaccines against rotavirus, varicella, and serogroup B and ACYW Neisseria meningitidis, France could become more vulnerable to some of these rebound effects.
researchgate.net [2022-11-21] Robert Cohen, Marion Ashman, ..., Emmanuelle Varon, ..., Emmanuel Grimprel, May 2021 link archive General
Receipt of influenza vaccination was not associated with virus interference among our population. Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus; however, significant protection with vaccination was associated not only with most influenza viruses, but also parainfluenza, RSV, and non-influenza virus coinfections. [Emphasis added]
[...]
nih.gov [2021-04-11] Greg G.Wolff, 10 January 2020 link archive General
Purpose: Receiving influenza vaccination may increase the risk of other respiratory viruses, a phenomenon known as virus interference. Test-negative study designs are often utilized to calculate influenza vaccine effectiveness. The virus interference phenomenon goes against the basic assumption of the test-negative vaccine effectiveness study that vaccination does not change the risk of infection with other respiratory illness, thus potentially biasing vaccine effectiveness results in the positive direction. This study aimed to investigate virus interference by comparing respiratory virus status among Department of Defense personnel based on their influenza vaccination status. Furthermore, individual respiratory viruses and their association with influenza vaccination were examined.
Results: We compared vaccination status of 2880 people with non-influenza respiratory viruses to 3240 people with pan-negative results. Comparing vaccinated to non-vaccinated patients, the adjusted odds ratio for non-flu viruses was 0.97 (95% confidence interval (CI): 0.86, 1.09; p = 0.60). Additionally, the vaccination status of 3349 cases of influenza were compared to three different control groups: all controls (N = 6120), non-influenza positive controls (N = 2880), and pan-negative controls (N = 3240). The adjusted ORs for the comparisons among the three control groups did not vary much (range: 0.46-0.51).
Conclusions: Receipt of influenza vaccination was not associated with virus interference among our population. Examining virus interference by specific respiratory viruses showed mixed results. Vaccine derived virus interference was significantly associated with coronavirus and human metapneumovirus; however, significant protection with vaccination was associated not only with most influenza viruses, but also parainfluenza, RSV, and non-influenza virus coinfections.
[...]
Table 5. Respiratory viruses and odds ratios by vaccination status.
' [...] To conclude, the injection of respiratory viral antigen or mrna that produced respiratory viral antigen leads to primary sensitization via IGE. Subsequent exposure to the antigen leads to an IGE mediated cytokine storm. There is cross immunity between Coronavirus vaccine and influenza vaccine with the coronavirus and influenza viral antigens. Treatment with allergy medications has been implemented. One such protocol was recently implemented by Dr. Chetty. An important additional medication for this mechanism of illness is cromolyn sodium which is available in liquid oral form and inhalation. It stabilizes mast cells and prevents the release of histamine. This should be added to the armamentarium of medications used.’
pubmed.ncbi.nlm.nih.gov [2022-10-21] Greg G Wolff, Jan 10, 2020 link archive General
Coronavirus disease (COVID-19) public health policy has focused on the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus and its effects on human health while environmental factors have been largely ignored. In considering the epidemiological triad (agent-host-environment) applicable to all disease, we investigated a possible environmental factor in the COVID-19 pandemic: ambient radiofrequency radiation from wireless communication systems including microwaves and millimeter waves. [...]
[...]
Relevance for Patients:
In short, WCR has become a ubiquitous environmental stressor that we propose may have contributed to adverse health outcomes of patients infected with SARS-CoV-2 and increased the severity of the COVID-19 pandemic. Therefore, we recommend that all people, particularly those suffering from SARS-CoV-2 infection, reduce their exposure to WCR as much as reasonably achievable until further research better clarifies the systemic health effects associated with chronic WCR exposure.
[...]
5. Conclusion
There is a substantial overlap in pathobiology between COVID-19 and WCR exposure. The evidence presented here indicates that mechanisms involved in the clinical progression of COVID-19 could also be generated, according to experimental data, by WCR exposure. Therefore, we propose a link between adverse bioeffects of WCR exposure from wireless devices and COVID-19.
[...]
ncbi.nlm.nih.gov [2021-12-05] Beverly Rubik and Robert R. Brown, September 29, 2021 link archive General
Electricity has shaped the modern world. But how has it affected our health and environment?
Over the last 220 years, society has evolved a universal belief that electricity is ‘safe’ for humanity and the planet. Scientist and journalist Arthur Firstenberg disrupts this conviction by telling the story of electricity in a way it has never been told before - from an environmental point of view - by detailing the effects that this fundamental societal building block has had on our health and our planet.
In The Invisible Rainbow, Firstenberg traces the history of electricity from the early eighteenth century to the present, making a compelling case that many environmental problems, as well as the major diseases of industrialised civilisation - heart disease, diabetes, and cancer - are related to electrical pollution.
Journalist Derrick Broze examines a recently published review article which claims a connection between symptoms of wireless radiation exposure and COVID19. This study is just the latest in similar claims over the last 2 years. Is there any truth to this latest paper? Find out in this video!
Please read and agree to the disclaimer before watching this video. . Spike Proteins In Immune Cells - Dr. Bruce Patterson Discusses COVID Long Haul
Dr. Bruce Patterson’s team has discovered that the S1 pieces of the spike proteins persist in the monocytes resulting in immune dysregulation and long-haul syndrome. Let’s discuss these findings with him.
New research from the Massachusetts General Hospital (MGH) and the National Institutes of Health hypothesizes nerve damage as the cause of long COVID symptoms in some people. The small study found treating patients with immunotherapies targeting the neuropathy could improve long COVID symptoms.
Scientists and doctors are continuing to grapple with the emergence of long COVID, a post-viral condition characterized by persistent symptoms of COVID-19. It is still unclear exactly what causes long COVID, how long the condition may last, and perhaps most importantly, how to treat the chronic illness.
[...]
The small new study followed 17 patients with a variety of long COVID symptoms. The researchers evaluated the patients for a condition known as peripheral neuropathy, a type of nerve damage signaled by pain in the hands or feet, weakness, fatigue and sensory changes.
The study found 59 percent of the long COVID patients could effectively fit a clinical diagnosis of peripheral neuropathy. Even more significantly, the researchers found treating some of the patients with immunotherapies used to target inflammatory neuropathy led to improvements in symptoms.
[...]
newatlas.com [2022-03-02] By Rich Haridy, March 01, 2022 link archive General
Del moderates an incredible panel of luminaries including Dr. Pierre Kory, Dr. Robert Malone, and Dr. Richard Urso, who unabashedly hit on the dangers of the Covid-19 vaccine and the broader, systemic issues that triggered a public health catastrophe.
thehighwire.com [2022-10-18] The HIGHWIRE, October 14, 2022 link archive General
Following a referral on 1 September 2022 from the Minister for Health and Aged Care, the Hon Mark Butler MP, the House Standing Committee on Health, Aged Care and Sport will inquire into and report on Long COVID and Repeated COVID Infections.
Submissions closed on 18 November 2022.
The evidence gathering phase of the inquiry is nearly complete and any final late submissions must be received by 20 February 2023.
aph.gov.au [2023-02-16] Submissions closed: 18 November 2022 link archive General
The Committee aims to publish as much inquiry evidence as possible, including by publishing submissions that may amount to misleading opinions about COVID-19. Ultimately, it is a Committee decision as to whether a particular submission is published. The Committee does not necessarily endorse the views contained within submissions published on this website.
Submissions received by the Committee
Submissions may be re-ordered by clicking on a column header. They may also be grouped by Organisation/Individual, State/Territory.
Background: Individuals with post-acute sequelae of COVID (PASC) may have a persistence in immune activation that differentiates them from individuals who have recovered from COVID without clinical sequelae. To investigate how humoral immune activation may vary in this regard, we compared patterns of vaccine-provoked serological response in patients with PASC compared to individuals recovered from prior COVID without PASC.
[...]
Results: Individuals with PASC mounted consistently higher post-vaccination IgG-S antibody levels when compared to COVID-recovered (median log IgG-S 3.98 versus 3.74, P < 0.001), with similar results seen for ACE2 binding levels (median 99.1 versus 98.2, P = 0.044). The post-vaccination IgM-S response in PASC was attenuated but persistently unchanged over time (P = 0.33), compared to in COVID recovery wherein the IgM-S response expectedly decreased over time (P = 0.002). Findings remained consistent when accounting for demographic and clinical variables including indices of index infection severity and comorbidity burden.
Conclusion: We found evidence of aberrant immune response distinguishing PASC from recovered COVID. This aberrancy is marked by excess IgG-S activation and ACE2 binding along with findings consistent with a delayed or dysfunctional immunoglobulin class switching, all of which is unmasked by vaccine provocation. These results suggest that measures of aberrant immune response may offer promise as tools for diagnosing and distinguishing PASC from non-PASC phenotypes, in addition to serving as potential targets for intervention.
IgG antibodies against the Spike protein may be associated with post-COVID/vaccine syndromes while antibodies (acute IgM, convalescent IgG) directed against the nucleocapsid and T-cell immunity may be protective against the prolonged syndrome(s). I have noticed in my practice that anti-Spike antibody levels are associated with the duration and severity of long-COVID-19 and vaccine injury syndromes. While the antibodies should have never been used as clinical surrogates to approve or extend EUA applications for vaccines (as the LabCorp disclaimer indicates), they are useful in identifying the frequent complications after the unwise injections.
pubmed.ncbi.nlm.nih.gov [2023-06-11] Sandy Joung, Brittany Weber, ..., Catherine N Le, Feb, 2023 link archive General
Studies probe unusual cases of neurologic complications, blood pressure swings, and other side effects
[...]
“You see one or two patients and you wonder if it’s a coincidence,” says Anne Louise Oaklander, a neurologist and researcher at Harvard Medical School. “But by the time you’ve seen 10, 20,” she continues, trailing off. “Where there’s smoke, there’s fire.”
Cases seem very rare—far less common than Long Covid after infection. Symptoms can include persistent headaches, severe fatigue, and abnormal heart rate and blood pressure. They appear hours, days, or weeks after vaccination and are difficult to study. But researchers and clinicians are increasingly finding some alignment with known medical conditions. One is small fiber neuropathy, a condition Oaklander studies, in which nerve damage can cause tingling or electric shock–like sensations, burning pain, and blood circulation problems. The second is a more nebulous syndrome, with symptoms sometimes triggered by small fiber neuropathy, called postural orthostatic tachycardia syndrome (POTS). It can involve muscle weakness, swings in heart rate and blood pressure, fatigue, and brain fog.
Patients with postvaccination symptoms may have features of one or both conditions, even if they don’t meet the criteria for a diagnosis. Both are also common in patients with Long Covid, where they’re often attributed to an immune overreaction.
Although more researchers are now taking Long Vax seriously, regulators in the United States and Europe say they have looked for, but have not found, a connection between COVID-19 vaccines and small fiber neuropathy or POTS. “We can’t rule out rare cases,” says Peter Marks, director of the U.S. Food and Drug Administration’s Center for Biologics Evaluation and Research, which oversees vaccines. “If a provider has somebody in front of them, they may want to take seriously the concept [of] a vaccine side effect,” he says. But Marks also worries about “the sensational headline” that could mislead the public, and he emphasizes that vaccine benefits far outweigh any risks.
Despite the uncertainties, German Minister of Health Karl Lauterbach acknowledged in March that though rare, Long Covid–like symptoms after vaccination are a real phenomenon. He said his ministry was working to organize funding for studies, although none has been announced so far.
Researchers studying these complications also worry about undermining trust in COVID-19 vaccines. Harlan Krumholz, a cardiologist at Yale University, says concern that the antivaccine movement would seize on any research findings made him hesitant at first to dive in. But about a year ago he and Yale immunologist Akiko Iwasaki began to welcome postvaccination patients into a new study called LISTEN that also includes Long Covid patients. Among other things, it aims to correlate symptoms with immune cell patterns in blood samples.
“I’m persuaded that there’s something going on” with these side effects, Krumholz says. “It’s my obligation, if I truly am a scientist, to have an open mind and learn if there’s something that can be done.”
SCIENCE FIRST wrote about these health concerns in January 2022, describing efforts by scientists at the National Institutes of Health to study and treat affected individuals. A study including 23 people was posted as a preprint in May 2022 but never published. Following Science’s story, almost 200 people contacted the journal sharing their postvaccination symptoms.
Research has since proceeded slowly. This is “a challenging outcome to monitor,” Tom Shimabukuro of the U.S. Centers for Disease Control and Prevention told a government advisory committee in January. Still, more than two dozen case studies have accumulated describing POTS or small fiber neuropathy following a COVID-19 shot, regardless of the vaccine manufacturer.
[...]
science.org [2023-07-05] GRETCHEN VOGEL, JENNIFER COUZIN-FRANKEL, 3 JUL 2023 link archive General
At least 5–10% of subjects surviving COVID-19 develop the post-COVID-19 condition (PCC) or “Long COVID”. The clinical presentation of PCC is heterogeneous, its pathogenesis is being deciphered, and objective, validated biomarkers are lacking. It is unknown if PCC is a single entity or a heterogeneous syndrome with overlapping pathophysiological basis. The large US RECOVER study identified four clusters of subjects with PCC according to their presenting symptoms. However, the long-term clinical implications of PCC remain unknown.
Methods
We conducted a 2-year prospective cohort study of subjects surviving COVID-19, including individuals fulfilling the WHO PCC definition and subjects with full clinical recovery. We systematically collected post-COVID-19 symptoms using prespecified questionnaires and performed additional diagnostic imaging tests when needed. Factors associated with PCC were identified and modelled using logistic regression. Unsupervised clustering analysis was used to group subjects with PCC according to their presenting symptoms. Factors associated with PCC recovery were modelled using a direct acyclic graph approach.
Findings
The study included 548 individuals, 341 with PCC, followed for a median of 23 months (IQR 16.5–23.5), and 207 subjects fully recovered. In the model with the best fit, subjects who were male and had tertiary studies were less likely to develop PCC, whereas a history of headache, or presence of tachycardia, fatigue, neurocognitive and neurosensitive complaints and dyspnea at COVID-19 diagnosis predicted the development of PCC. The cluster analysis revealed the presence of three symptom clusters with an additive number of symptoms. Only 26 subjects (7.6%) recovered from PCC during follow-up; almost all of them (n = 24) belonged to the less symptomatic cluster A, dominated mainly by fatigue. Recovery from PCC was more likely in subjects who were male, required ICU admission, or had cardiovascular comorbidities, hyporexia and/or smell/taste alterations during acute COVID-19. Subjects presenting with muscle pain, impaired attention, dyspnea, or tachycardia, conversely, were less likely to recover from PCC.
Interpretation
Preexisting medical and socioeconomic factors, as well as acute COVID-19 symptoms, are associated with the development of and recovery from the PCC. Recovery is extremely rare during the first 2 years, posing a major challenge to healthcare systems.
Researchers want to see "internationally established" diagnostic criteria when it comes to long COVID, as well as narrowly defined symptoms and the avoidance of the "umbrella term".
The risk of contracting long COVID may have been exaggerated due to flawed research, leading to unnecessarily high levels of anxiety about suffering from it, a new study has suggested.
"Major flaws" in the literature on the condition likely exaggerated the true threat of contracting it, the new research argues.
[...]
Now, researchers from the UK, along with Denmark and the USA, say "many scientific publications" overestimated the prevalence of long COVID because of "overly broad definitions, lack of control groups, inappropriate control groups, and other methodological flaws".
Instead, the authors of the new study argue that the symptoms are common among upper respiratory viruses.
The research team said this lack of definition could end up leading to an increase in healthcare spending and more anxiety, as well as misdiagnoses and a diversion of funds.
Concerns about too many symptoms and no required link to COVID
Published in the British Medical Journal's Evidence-Based Medicine, the new paper looked at the definition of the condition by several global health organisations - including the National Institute for Health and Care Excellence (NICE) and the World Health Organisation (WHO).
The study argues none of the definitions "requires a causal link" to COVID-19 infection, adding any symptoms that happen after a confirmed or suspected infection could be considered consistent with long COVID.
"In general, in the scientific literature, imprecise definitions have resulted in more than 200 symptoms being associated with the condition termed long COVID," the researchers said.
Researchers also said the studies in the early stages of the pandemic are more likely to have included fewer patients with mild or no symptoms, which could have led to a sampling bias.
They said: "Our analysis indicates that, in addition to including appropriately matched controls, there is a need for better case definitions and more stringent (long COVID) criteria, which should include continuous symptoms after confirmed SARS-CoV-2 infection and take into consideration baseline characteristics, including physical and mental health, which may contribute to an individual's post-COVID experience."
Background: Autoimmunity has been reported in patients with severe coronavirus disease 2019 (COVID-19). We investigated whether anti-nuclear/extractable-nuclear antibodies (ANAs/ENAs) were present up to a year after infection, and if they were associated with the development of clinically relevant post-acute sequalae of COVID-19 (PASC) symptoms.
Methods: A rapid-assessment line immunoassay was used to measure circulating levels of ANAs/ENAs in 106 convalescent COVID-19 patients with varying acute phase severities at 3, 6 and 12 months post-recovery. Patient-reported fatigue, cough and dyspnoea were recorded at each time point. Multivariable logistic regression model and receiver operating curves were used to test the association of autoantibodies with patient-reported outcomes and pro-inflammatory cytokines.
Results: Compared to age- and sex-matched healthy controls (n=22) and those who had other respiratory infections (n=34), patients with COVID-19 had higher detectable ANAs at 3 months post-recovery (p<0.001). The mean number of ANA autoreactivities per individual decreased between 3 and 12 months (from 3.99 to 1.55) with persistent positive titres associated with fatigue, dyspnoea and cough severity. Antibodies to U1-snRNP and anti-SS-B/La were both positively associated with persistent symptoms of fatigue (p<0.028, area under the curve (AUC) 0.86) and dyspnoea (p<0.003, AUC=0.81). Pro-inflammatory cytokines such as tumour necrosis factor (TNF)-α and C-reactive protein predicted the elevated ANAs at 12 months. TNF-α, D-dimer and interleukin-1β had the strongest association with symptoms at 12 months. Regression analysis showed that TNF-α predicted fatigue (β=4.65, p=0.004) and general symptomaticity (β=2.40, p=0.03) at 12 months.
Interpretation: Persistently positive ANAs at 12 months post-COVID are associated with persisting symptoms and inflammation (TNF-α) in a subset of COVID-19 survivors. This finding indicates the need for further investigation into the role of autoimmunity in PASC.
Test for Auto-Immunity is Positive in Patients with Respiratory Long-COVID
Among an array of tests I obtain in patients with post-acute sequelae after SARS-CoV-2 infection or COVID-19 vaccine is the antinuclear antibody. First described in 1948, ANA identification has been the foundation of diagnosis for autoimmune connective tissue disease, including systemic lupus erythematosus (SLE), Sjogren's syndrome, and polymyositis/dermatomyositis.
Before the pandemic, I have found most ANA positive syndromes responsive to chronic hydroxychloroquine therapy among other agents. It is interesting that HCQ became one of several choices in the standard of care for the early ambulatory management of high-risk COVID-19 as established by the McCullough Protocol.
Son et al, evaluated severe COVID-19 cases, many of whom were hospitalized early in the pandemic and found that research grade ANA assays were positive in a large fraction with persistent respiratory and chest symptoms such as fatigue, cough, and dyspnea. Their findings suggest SARS-CoV-2 infection itself induces auto-immunity, particularly with severe infections.
While there are no randomized trials of HCQ in long-COVID, it has been my observation that ANA positive patients improve on HCQ when they are suffering from post-acute sequalae after SARS-CoV-2 infection and/or COVID-19 vaccination. So don’t be surprised if you see patients taking HCQ on a longer-term basis as they recover through the pandemic.
These data suggest Biden’s Office of Long COVID Research and Practiceshould focus on the generic drugs we were finding useful for acute treatment including HCQ, IVM, colchicine, etc. Instead the disastrous research program has spent $1B and produced no new therapies or protocols for patients suffering in the community.
pubmed.ncbi.nlm.nih.gov [2023-11-18] Kiho Son, Rameen Jamil, ..., Manali Mukherjee, January 2023 link archive General
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can lead to postacute sequelae in multiple organ systems, but evidence is mostly limited to the first year postinfection. We built a cohort of 138,818 individuals with SARS-CoV-2 infection and 5,985,227 noninfected control group from the US Department of Veterans Affairs and followed them for 2 years to estimate the risks of death and 80 prespecified postacute sequelae of COVID-19 (PASC) according to care setting during the acute phase of infection. The increased risk of death was not significant beyond 6 months after infection among nonhospitalized but remained significantly elevated through the 2 years in hospitalized individuals. Within the 80 prespecified sequelae, 69% and 35% of them became not significant at 2 years after infection among nonhospitalized and hospitalized individuals, respectively. Cumulatively at 2 years, PASC contributed 80.4 (95% confidence interval (CI): 71.6–89.6) and 642.8 (95% CI: 596.9–689.3) disability-adjusted life years (DALYs) per 1,000 persons among nonhospitalized and hospitalized individuals; 25.3% (18.9–31.0%) and 21.3% (18.2–24.5%) of the cumulative 2-year DALYs in nonhospitalized and hospitalized were from the second year. In sum, while risks of many sequelae declined 2 years after infection, the substantial cumulative burden of health loss due to PASC calls for attention to the care needs of people with long-term health effects due to SARS-CoV-2 infection.
? Somebody on the UK Mirror’s editorial staff must miss the good old days of hyperbolic covid doom headlines. Check out this time-traveling headline of hysteria that splashed down in August (though nobody noticed):
It’s a little stale but I thought it was worth mentioning since this study and the outrageous Mirror headline — Urgent Death Warning! — made the rounds on social media this week, supposedly to prove how deadly ‘long covid’ is or something.
The study referenced in the Mirror article published in Nature Medicine back on August 21st with the bland title, “Postacute sequelae of COVID-19 at 2 years.” As you can probably guess, nothing in the study justifies any “urgent death warning,” whatever that is. The researchers studied 140,000 VA patients and found a slightly elevated risk of death for six months following mild covid infection, and a higher (+14%) risk following hospitalization for covid infection lasting for two years (and running, since that’s when the study ended).
It wasn’t just death; that’s just what the Mirror focused on. The researchers allegedly found a higher risk for most (60%) of a very long list of problems they called “postacute sequelae.” It's such an impressively-gigantic list that I though it would be easier to just show you the study’s chart:
The chart shows the relative risks of each health issue by the number of days after infection (30–90, 91–180, 181–360, 361–540 and 541–720). The days are counterintuitively labeled at the bottom of the chart, by the last day of each time period. The two rows shown for each health issue are: the top row is extra risks for folks who got mild covid (85%), and the bottom row is for folks hospitalized for serious covid (15%). Red is bad, green is good.
In my experience as a lawyer during the pandemic, the Veteran’s Administration refused to treat veterans — making them ‘patients’ — unless they were jabbed. So it’s fair to assume all 140,000 VA patients in this study drank the mRNA cocktail (or were coerced). So the study’s conclusion only applies to jabbed people, which unintentionally makes it specially interesting: There seems to be some good news for jabbed people in the data.
I’ve learned to start reviewing studies at the ethics disclosures. Check out this list of notable authors:
B.B. reports receiving consultation fees from AstraZeneca. Z.A.A. reports receiving consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. Z.A.A. and Y.X. report consulting (uncompensated) for Pfizer.
Haha, my favorite one was Y.X. — Yan Xie — who apparently consults for Pfizer for free. He’s a volunteer! Of course these whitecoat volunteers are trying to help blame all these health problems on long covid, so that nothing else gets the blame. That would be unfortunate.
The following three facts tell you everything you need to know about the study’s stated conclusions: (1) it only included vaccinated people, (2) its author list was stacked with pharma professionals, and (3) it only included patients who came in for their covid infections.
With those facts in mind, there’s nothing alarming about this study, which seems more designed as cover for defective vaccine products. But when viewed as a study of jabbed people’s enhanced risk of side effects, we see the risks definitely taper off over a 24-month period.
First of all, that suggests the mRNA’s harmful effects do eventually wear off, or the body learns to cope with them somehow. So that’s good.
Second, the worst risks of side effects appear among people who responded the worst to a covid infection and were subsequently hospitalized. Serious covid thus appears to be a kind of litmus test for which risk category a jabbed person falls into. If they recover from their (repeated) mild covid infections at home, this study suggests their risks of other side effects may also be relatively lower.
Both possible conclusions are potential good news for jab takers. True, too many of the excess health risks still remain elevated at 24 months, which is troubling. But the trend seems to be going the right way, if this data is reliable.
Finally, I’d like to point out the hysterical double-standard at play here. If you showed one of these medical fetishists data plotting higher adverse cardiac events within 48 hours of injection, they’d scream — at the top of their lungs — correlation does not equal causation! But lookie here, in their study they conclude, without even trying to prove a mechanism, just treating it were an established fact, that the covid virus caused all these other sequelae in a 100% jabbed population. Correlated! Caused! Ha!
nature.com [2023-12-14] Benjamin Bowe, Yan Xie, Ziyad Al-Aly, 21 August 2023 link archive General
Background: Long COVID or long-term symptoms after COVID-19 has the ability to affect health and quality of life. Knowledge about the burden and predictors could aid in their prevention and management. Most of the studies are from high-income countries and focus on severe acute COVID-19 cases. We did this study to estimate the incidence and identify the characteristics and predictors of Long COVID among our patients.
Methodology: We recruited adult (≥18 years) patients who were diagnosed as Reverse Transcription Polymerase Chain Reaction (RTPCR) confirmed SARS-COV-2 infection and were either hospitalized or tested on outpatient basis. Eligible participants were followed up telephonically after four weeks and six months of diagnosis of SARS-COV-2 infection to collect data on sociodemographic, clinical history, vaccination history, Cycle threshold (Ct) values during diagnosis and other variables. Characteristics of Long COVID were elicited, and multivariable logistic regression was done to find the predictors of Long COVID.
Results: We have analyzed 487 and 371 individual data with a median follow-up of 44 days (Inter quartile range (IQR): 39,47) and 223 days (IQR:195,251), respectively. Overall, Long COVID was reported by 29.2% (95% Confidence interval (CI): 25.3%,33.4%) and 9.4% (95% CI: 6.7%,12.9%) of participants at four weeks and six months of follow-up, respectively. Incidence of Long COVID among patients with mild/moderate disease (n = 415) was 23.4% (95% CI: 19.5%,27.7%) as compared to 62.5% (95% CI: 50.7%,73%) in severe/critical cases(n = 72) at four weeks of follow-up. At six months, the incidence among mild/moderate (n = 319) was 7.2% (95% CI:4.6%,10.6%) as compared to 23.1% (95% CI:12.5%,36.8%) in severe/critical (n = 52). The most common Long COVID symptom was fatigue. Statistically significant predictors of Long COVID at four weeks of follow-up were-Pre-existing medical conditions (Adjusted Odds ratio (aOR) = 2.00, 95% CI: 1.16,3.44), having a higher number of symptoms during acute phase of COVID-19 disease (aOR = 11.24, 95% CI: 4.00,31.51), two doses of COVID-19 vaccination (aOR = 2.32, 95% CI: 1.17,4.58), the severity of illness (aOR = 5.71, 95% CI: 3.00,10.89) and being admitted to hospital (Odds ratio (OR) = 3.89, 95% CI: 2.49,6.08).
Conclusion: A considerable proportion of COVID-19 cases reported Long COVID symptoms. More research is needed in Long COVID to objectively assess the symptoms and find the biological and radiological markers.
Background and Objectives: After recovering from COVID-19, patients may experience persistent symptoms, known as post-COVID-19 syndrome or long COVID, which include a range of continuing health problems. This research explores the prevalence, associated factors, and overall health outcomes of long COVID during a period of extensive vaccination and antiviral treatment availability in Thailand. Materials and Methods: This observational study involved 390 adult patients with COVID-19 between January and March 2022. Beginning three months after their diagnosis, these patients were interviewed via telephone every three months for a period of one year. The data collection process included gathering demographic information and administering a standardized questionnaire that addressed the patients’ physical condition following COVID-19, their mental health, sleep disturbances, and overall quality of life. Results: The cohort consisted of 390 participants, with an average age of 31.8 ± 13.6. Among them, 96.7% (n = 377) were vaccinated, and 98.2% (n = 383) underwent antiviral treatment. Long-COVID prevalence was observed at 77.7%, with the most frequently reported symptoms being fatigue (64.1%) and cough (43.9%). Regarding mental health, depression was reported by 8.2% of the participants, anxiety by 4.1%, and poor sleep quality by 33.3%. Advanced statistical analysis using multivariable logistic regression showed significant links between long-COVID symptoms and patients aged below 60 (p = 0.042), as well as the initial symptom of cough (p = 0.045). In the subset of long-COVID sufferers, there was a notable correlation in females with symptoms such as headaches (p = 0.001), dizziness (p = 0.007), and brain fog (p = 0.013). Conclusions: Despite the extensive distribution of vaccines and antiviral therapies, the prevalence of long COVID remains high, being associated particularly with individuals under 60 and those exhibiting a cough as an early symptom. The study further reveals that mental health issues related to long COVID are profound, going beyond the scope of physical symptomatology.
Millions of Americans are still suffering months or even years after they were infected with COVID. Long COVID as it’s commonly known is a serious and poorly understood problem. But there is also growing evidence that the COVID vaccine could cause a similar disease.
We need our government health agencies to take a serious look at this condition and stop stigmatizing doctors and patients who report these findings so we can get people the help they need.
We are critical care physicians with the FLCCC Alliance (the Front Line COVID-19 Critical Care Alliance) who have treated COVID patients throughout the pandemic. One of us recently opened a private practice focused on patients with long COVID.
In two years, the practice has evaluated and treated over 1,000 individuals. Approximately 70 percent of these patients said their reported symptoms occurred in the minutes, hours, days and weeks after COVID vaccination, as opposed to after COVID infection. This could be tied to a new condition that’s flown under the radar until recently.
This syndrome, dubbed “long vax,” is just starting to make its way into the medical literature. Dr. Harlan Krumholz at the Yale School of Medicine published a survey of 241 patients who described post-COVID vaccination symptoms of exercise intolerance, excessive fatigue, numbness, brain fog and neuropathy, a nervous system disorder that can cause pain, tingling sensations, numbness or weakness. Long COVID patients were excluded from the study, which is now undergoing peer review.
The concern is that our findings, Krumholz’s study, and any reports of adverse events from COVID-19 vaccination, will be subject to the same institutional censorship we saw throughout the pandemic. Suppressing this information risks creating an even bigger disaster.
America’s health agencies need to snap into action to help study this problem so we can better understand and treat these conditions. Unfortunately, there doesn’t seem to be much hope of this happening. The National Institutes of Health is fixated on studying the effect of Paxlovid, an antiviral COVID treatment, to treat long COVID and long vax, despite it having no proven effect on autoimmune disease.
I found it very encouraging and a great sign of progress the Hill agreed to publish the op-ed. In their article, the doctors quickly got to the point: Dr. Kory and Dr. Marik reported they’ve been treating a whole lot of ‘long covid’ patients through their FLCCC organization, but they aren’t sure it is long covid:
In two years, our practice has evaluated and treated over 1,000 individuals (for ‘long covid’). Approximately 70 percent of these patients said their reported symptoms occurred in the minutes, hours, days and weeks after COVID vaccination, as opposed to after COVID infection. This could be tied to a new condition that’s flown under the radar until recently.
The docs next cited a new Yale study that is currently pending peer review. In the study, researchers looked at 241 patients experiencing what they called “post-vaccination syndrome.” In other words, there’s even a clinical name for it now. (As usual, the Yale study included the increasingly rare but still obligatory jab endorsement claiming — without evidence — that PVS happens less often than long covid. So.)
The Scientific American article explained that a broad range of incurable autoimmune diseases — over 100 kinds — have suddenly, unexpectedly, and bafflingly surged to epidemic levels:
Autoimmunity is an epidemic. Most autoimmune diseases are being diagnosed in increasing numbers ranging from 3 to 12 percent annually across the globe. (Americans) could now have about a one in five chance of developing an autoimmune disease. The odds are greater for women, those with a genetic predisposition to autoimmunity, or those exposed to certain pollutants. These diseases include more than 100 lifelong and costly illnesses such as type 1 diabetes, rheumatoid arthritis, lupus and multiple sclerosis. They are often difficult to diagnose and currently impossible to cure.
The doctors mentioned that, unlike long covid, autoimmunity is measurable. They can test for looming autoimmune problems, by testing for autoantibodies, which are antibodies programmed to attack the person’s own cells and organs, rather than programmed to attack some kind of invasive bacteria or virus:
Autoantibodies are markers for the presence, or the possible development, of autoimmune diseases. We are finding more people with autoantibodies—immune system proteins that, instead of ignoring our cells and organs, treat them as invaders.
Now, I’m just a lawyer and not an immune specialist, but I wonder if these researchers considered the possibility that the autoantibodies may be targeting people’s own cells because they were transfected with spike protein mRNA?
I’m only asking.
The researchers noted the fact that, one year before on December 29, 2022, the Biden Administration quietly and very timely set up a new Office of Autoimmune Research within the NIH. So they either saw the trend or knew it was coming.
Mainstream media is happen to drown us in propaganda about a flu epidemic but they have nothing to say about an autoimmune epidemic. Oh well. La, la, la, la, everything is going great!
thehill.com [2024-03-10] PIERRE KORY, PAUL MARIK, 03/06/24 link archive General
Millions worldwide experience post-acute sequelae of COVID-19 (PASC or long COVID), according to the World Health Organization (WHO), European Union and the UK and US governments.1–3 Long COVID symptoms >12 weeks after the initial severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection affecting 2–20% of patients with mild and severe acute COVID-19 are endemic in every jurisdiction with a competent health reporting system.1 Although the Australian Bureau of Statistics and other health agencies in Australia do not survey the prevalence of long COVID, it is estimated that it affects hundreds of thousands,2 presaging a parliamentary inquiry into long COVID4 and repeated SARS-CoV-2 infection,5 which reported to Federal Government in April 2023.6 The 566 submissions to the Inquiry, including those from states, territories, professional bodies and the public, largely concur with the view that long COVID presents health management and sociological challenges to Australian society (conspicuously, the Queensland Government has a somewhat different perspective, attributing long COVID to a predominantly nocebo effect7). Furthermore, the submissions recognise significant wellbeing and financial challenges to individuals with long COVID.
Long COVID is a heterogeneous disease with variable cardiac, pulmonary, haematological and neurological involvement in which investigation of patient-reported symptoms is frequently unremarkable. Long COVID’s overlap with myalgic encephalomyelitis/chronic fatigue syndrome, postural orthopaedic tachycardia syndrome (POTS) and other post-viral manifestations8 predisposes to a diagnosis by exclusion.9,10
There is no consensus on what causes lingering COVID-19 symptoms long after the acute infection has cleared.7 Indeed, there is no definition of what long COVID is. At present, public health officials are flying blind when it comes to long COVID and vaccination.11
Often unable to secure a diagnosis, patients are wont to seek multiple serial medical opinions, frequently being told their condition is due to anxiety or post-pandemic mental issues.8
The median duration of long COVID symptoms is five months, but 10% of patients still experience symptoms at 12 months.12 Fatigue, shortness of breath and difficulty concentrating are reported at least up to two years after SARS-CoV-2 infection.13 It is still too early to say whether some individuals with long COVID might never recover.
Long COVID patients present elevated inflammatory biomarkers (eg interleukin-6, C-reactive protein, tumour necrosis factor-α), which might function as a core set of blood biomarkers that can be used to diagnose and manage long COVID patients in clinical practice.14,15
Those subscribing to long COVID digital support groups report months of frustration at not being listened to, finding the health system woefully inadequate, with few primary or secondary care professionals knowing enough to offer much. The outcome for some of those experiencing long COVID is self-prescribed medication using over-the-counter remedies and dietary changes16 based on potentially conflicting or misleading online information.17 Some speak of a substantial proportion of their income being used in this way.4
Meanwhile, jobs, careers, incomes, community involvements, friendships, relationships, hope for a recovery and mental health are being destroyed. Those experiencing long COVID report that the long COVID digital support group is the ‘… only place they feel safe to share, the only place they feel understood, accepted, [and] supported’.4
One in five of those experiencing long COVID in the UK stopped working and was not back to work six months after disease onset.18 In Australia, an estimated 240,000 of those with long COVID no longer work full time.4 Work absenteeism might significantly impact the nation’s economy, as in the UK.19 In the US, long COVID has been declared a national emergency.20
Reduced to working part time to cope with unwellness, those with long COVID commonly report having to wait a year or more before receiving a diagnosis.4 Without a definitive diagnosis, those with long COVID are not eligible for Job Seeker, the Disability Support Pension and National Disability Insurance Scheme (NDIS) protection under the Fair Work Act, thereby conferring long-term financial difficulties for themselves and their dependents. There is a need for guidelines on how those with long COVID can access social security and employment protection.
Primary healthcare providers need more guidance from the Federal and State Health Department authorities on handling the long COVID deluge,4 and need to be educated on how to diagnose long COVID and best support those with the condition. Although some states have established long COVID clinics, some of these at least are of little help to the patient in providing substantive treatment guidelines or support and are little more than incident report centres. The waiting time for a long COVID clinic is typically several months or more.4 Some general practitioners (GPs) were unaware of the clinics’ existence in their area (R Tindle, pers. obs.). Clinics should be a resource to primary health providers, contribute to treatment plans and be able to refer to specialists.4 Clinical management, including mental health, should be codesigned with patients’ lived experiences. Specialised long COVID clinics now operate in numerous European countries; 1500 patients per week are referred to UK long COVID clinics, which provide online recovery platforms, hubs for children and GP training.21
There is concern that COVID-19 vaccination per se might contribute to long COVID, giving rise to the colloquial term ‘Long Vax(x)’.22 The spike protein of SARS-CoV-2 exhibits pathogenic characteristics and is a possible cause of post-acute sequelae after SARS-CoV-2 infection or COVID-19 vaccination. COVID-19 vaccines utilise a modified, stabilised prefusion spike protein that might share similar toxic effects with its viral counterpart.22,23 A possible association between COVID-19 vaccination and the incidence of POTS has been demonstrated in a cohort of 284,592 COVID-19-vaccinated individuals, though at a rate that was one-fifth of the incidence of POTS after SARS-CoV-2 infection.24 Multiple studies have shown an increased risk of myocarditis after vaccination with mRNA encoding SARS-CoV-2 spike protein.25–27 mRNA vaccines can result in spike protein expression in muscle tissue, the lymphatic system, cardiomyocytes and other cells after entry into the circulation.28 Recipients of two or more injections of the mRNA vaccines display a class switch to IgG4 antibodies. Abnormally high levels of IgG4 might cause autoimmune diseases, promote cancer growth, autoimmune myocarditis and other IgG 4-related diseases (IgG4-RD) in susceptible individuals.29 There are clear implications for vaccine boosting where these and similar observations8,22,30 relating to COVID-19 vaccination and the incidence of long COVID-like symptoms are substantiated, adding further to public health officials’ concerns. Understanding the persistence of viral mRNA and viral protein and their cellular pathological effects after vaccination with and without infection is clearly required. Because COVID-19 vaccines were approved without long-term safety data and might cause immune dysfunction, it is perhaps premature to assume that past SARS-CoV-2 infection is the sole common factor in long COVID.8 The Australian Government’s promise of $50 million from the Medical Research Future Fund for long COVID research31 will hopefully foment nationally coordinated long COVID and COVID-19 research programs encompassing basic science through to models of care.6 The proposed development of a national centre for disease control6 providing a national interrogative repository for hitherto fragmented incidence and outcome data for long COVID will aid in these investigations.
The April edition of The Australian Journal of General Practice included a viewpoint article that gently peeled off the vaccine band aid, titled “Long COVID Sufferers can take heart.”
The Australian Journal of General Practice (the AJGP) is a peer-reviewed medical journal published by The Royal Australian College of General Practitioners. It is a well-respected journal indexed in all the major sci/med databases, and it is widely read by Australian doctors in general practice.
The article’s main point — perhaps cleverly — was aimed at long covid, which one suspects is a problem that lots of Australian GPs are encountering in their practices. The article poignantly described the baffling syndrome:
Those subscribing to long COVID digital support groups report months of frustration at not being listened to, finding the health system woefully inadequate, with few primary or secondary care professionals knowing enough to offer much. The outcome for some of those experiencing long COVID is self-prescribed medication using over-the-counter remedies and dietary changes based on potentially conflicting or misleading online information. Some speak of a substantial proportion of their income being used in this way.
Meanwhile, jobs, careers, incomes, community involvements, friendships, relationships, hope for a recovery and mental health are being destroyed.
Just like the vaccine injured! But I digress.
Long covid is becoming big business. In the US, the NIH is swimming in long covid research money. Last year, in 2023, big long covid bucks flowed like water (headline from Stat News):
Results? Haha, results. Good one. But don’t worry, the NIH continues spending massive amounts of your money. Just this year (from the NIH’s website):
An infusion! Get it? Anyway, according to NIH, scientists remain baffled. But a lot of good little NIH-compliant, white-coated doggies are getting grant snacks, to diligently do studies, produce unparalled data, and publish useless long covid papers that blame everything but the jabs:
Nearly 90,000 adults and children are participating in NIH RECOVER observational studies through more than 300 clinical research sites across the country. The amount of data being produced is unparalleled compared to any program in the world. Recent RECOVER studies have found that severe cases of COVID-19 can change which genes are turned on or off(link is external) in certain stem cells; that individuals with comorbid conditions, such as HIV, may have more severe long-lasting symptoms(link is external) following COVID-19 infection; that virus can persist in tissues for many months, perhaps years(link is external), following initial infection; and there may be changes in the immune system(link is external) in people with Long COVID.
NIH expects this investment of time and resources in building a research program of this scale, scope and rigor will increase the odds in finding treatments that work.
Is it just me, or did that last sentence sound, well, not super confident? After spending nearly two billion dollars — just by the NIH — can we do no better than merely “increasing the odds” of finding a useful treatment?
Anyway, let’s return to this week’s Australian AJGP article. After setting the long covid table, and right before revealing the promised hope for long covid sufferers, the AJGP article suddenly switched to the vaccines in a monolithic, long, heavily footnoted paragraph (I highlighted some parts for you):
How about that? What might the average Australian general practitioner, carefully scanning the article to uncover a hope to tell her long covid patients about, make of that paragraph, which probably challenges everything she thought she knew about the jabs?
Some GPs will surely ignore that carefully researched paragraph. But one hopes it would shock and surprise others.
The article’s author packaged all that vaccine truth extremely carefully, allowing the AJGP’s editors comfort letting that one paragraph of jab criticism slip through, and while dangling the promise of an effective treatment to generate interest. Well done.
The terrific Dr. Campbell analyzed the AJGP op-ed in a recent video podcast, if you’d enjoy his take. Just be aware the vaxx problems described in the paragraph above were citations to prior studies, not any unique finding by this op-ed, a minor distinction that may not be competely clear in John’s video:
In terms of a single cohort, my guess would be that general practitioners probably represent the largest single group of medical professionals in Australia. As mentioned, “long covid” is probably a hot topic these days for general practitioners. So this article seems likely to be widely read.
Even though it wasn’t aimed at a large-audience of the general public, this article was aimed at a large audience of medical professionals who most need to hear that information. So this one wasn’t just a drip of vaccine truth, it was a gush.
www1.racgp.org.au [2024-04-13] Robert Tindle, April 2024 link archive General
Data on pathologic changes of the 2019 novel coronavirus disease (COVID-19) are scarce. To gain knowledge about the pathology that may contribute to disease progression and fatality, we performed postmortem needle core biopsies of lung, liver, and heart in four patients who died of COVID-19 pneumonia. The patients’ ages ranged from 59 to 81, including three males and one female. Each patient had at least one underlying disease, including immunocompromised status (chronic lymphocytic leukemia and renal transplantation) or other conditions (cirrhosis, hypertension, and diabetes). Time from disease onset to death ranged from 15 to 52 days. All patients had elevated white blood cell counts, with significant rise toward the end, and all had lymphocytopenia except for the patient with leukemia. Histologically, the main findings are in the lungs, including injury to the alveolar epithelial cells, hyaline membrane formation, and hyperplasia of type II pneumocytes, all components of diffuse alveolar damage. Consolidation by fibroblastic proliferation with extracellular matrix and fibrin forming clusters in airspaces is evident. In one patient, the consolidation consists of abundant intra-alveolar neutrophilic infiltration, consistent with superimposed bacterial bronchopneumonia. The liver exhibits mild lobular infiltration by small lymphocytes, and centrilobular sinusoidal dilation. Patchy necrosis is also seen. The heart shows only focal mild fibrosis and mild myocardial hypertrophy, changes likely related to the underlying conditions. In conclusion, the postmortem examinations show advanced diffuse alveolar damage, as well as superimposed bacterial pneumonia in some patients. Changes in the liver and heart are likely secondary or related to the underlying diseases.
[...]
The main pathologic findings from the lungs of these fatal cases of COVID-19 pneumonia include hyaline membrane formation, fibrin exudates, epithelial damage, and diffuse type II pneumocyte hyperplasia, which are all features of DAD. Mild thickening of alveolar walls is also evident in some cases, suggesting a more advanced stage. However, mature fibrosis is not seen. A common feature of the chest radiological findings of COVID-19 pneumonia is GGO, which may represent an early exudative phase of COVID-19 pneumonia. [...]
nature.com [2022-08-04] Sufang Tian, Yong Xiong, ..., 14 April 2020 link archive General
Rationale: The incidence and sites of mucus accumulation andmolecular regulation of mucin gene expression in coronavirus (COVID-19) lung disease have not been reported.
Objectives: To characterize the incidence of mucusaccumulation and the mechanisms mediating mucinhypersecretion in COVID-19 lung disease.
[...]
Conclusions: SARS-CoV-2 infection is associated with a highprevalence of distal airspace mucus accumulation and increasedMUC5B expression in COVID-19 autopsy lungs. HBE culturestudies identified roles for EGFR and IL-1R signaling in mucingene regulation after SARS-CoV-2 infection. These data suggestthat time-sensitive mucolytic agents, specific pathway inhibitors,or corticosteroid administration may be therapeutic forCOVID-19 lung disease.
[...]
atsjournals.org [2022-12-14] Takafumi Kato, Takanori Asakura, ..., Richard C. Boucher, December 1, 2022 link archive General
Bacterial and fungal co-infections are reported complications of coronavirus disease 2019 (COVID-19) in critically ill patients but may go unrecognized premortem due to diagnostic limitations. We compared the premortem with the postmortem detection of pulmonary co-infections in 55 fatal COVID-19 cases from March 2020 to March 2021. The concordance in the premortem versus the postmortem diagnoses and the pathogen identification were evaluated. Premortem pulmonary co-infections were extracted from medical charts while applying standard diagnostic definitions. Postmortem co-infection was defined by compatible lung histopathology with or without the detection of an organism in tissue by bacterial or fungal staining, or polymerase chain reaction (PCR) with broad-range bacterial and fungal primers. Pulmonary co-infection was detected premortem in significantly fewer cases (15/55, 27%) than were detected postmortem (36/55, 65%; p < 0.0001). Among cases in which co-infection was detected postmortem by histopathology, an organism was identified in 27/36 (75%) of cases. Pseudomonas, Enterobacterales, and Staphylococcus aureus were the most frequently identified bacteria both premortem and postmortem. Invasive pulmonary fungal infection was detected in five cases postmortem, but in no cases premortem. According to the univariate analyses, the patients with undiagnosed pulmonary co-infection had significantly shorter hospital (p = 0.0012) and intensive care unit (p = 0.0006) stays and significantly fewer extra-pulmonary infections (p = 0.0021). Bacterial and fungal pulmonary co-infection are under-recognized complications in critically ill patients with COVID-19.
Inpatient COVID-19 protocol-driven care has been heavily criticized for being nihilistic, use of unsafe and ineffective remdesivir, and cruel in it’s treatment of patients and families. Now a new concern has been brought forward by the National Institutes of Health Autopsy Consortium—secondary bacterial and in some cases invasive fungal infections not recognized clinically before death.
Platt et al summarized autopsy findings in 55 fatal cases where death occurred on average 18 days after admission to the hospital.
“Pulmonary co-infection was detected premortem in significantly fewer cases (15/55, 27%) than were detected postmortem (36/55, 65%; p < 0.0001). Among cases in which co-infection was detected postmortem by histopathology, an organism was identified in 27/36 (75%) of cases. Pseudomonas, Enterobacter, and Staphylococcus aureus were the most frequently identified bacteria both premortem and postmortem. Invasive pulmonary fungal infection was detected in five cases postmortem, but in no cases premortem.”
In 44% of the missed cases, there was no appropriate antimicrobial coverage for a hospital acquired pneumonia. Thus, this is another deficiency of hospital care and an area for critical review of historical cases and improvement in the care of future ones.
pubmed.ncbi.nlm.nih.gov [2023-12-12] Andrew P Platt, Benjamin T Bradley, ..., Daniel S Chertow, July 2023 link archive General
Severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2)-induced infection, the cause of coronavirus disease 2019 (COVID-19), is characterized by acute clinical pathologies, including various coagulopathies that may be accompanied by hypercoagulation and platelet hyperactivation. Recently, a new COVID-19 phenotype has been noted in patients after they have ostensibly recovered from acute COVID-19 symptoms. This new syndrome is commonly termed Long COVID/Post-Acute Sequelae of COVID-19 (PASC). Here we refer to it as Long COVID/PASC. Lingering symptoms persist for as much as 6 months (or longer) after acute infection, where COVID-19 survivors complain of recurring fatigue or muscle weakness, being out of breath, sleep difficulties, and anxiety or depression. Given that blood clots can block microcapillaries and thereby inhibit oxygen exchange, we here investigate if the lingering symptoms that individuals with Long COVID/PASC manifest might be due to the presence of persistent circulating plasma microclots that are resistant to fibrinolysis.
[...]
Results
We show that plasma samples from Long COVID/PASC still contain large anomalous (amyloid) deposits (microclots). We also show that these microclots in both acute COVID-19 and Long COVID/PASC plasma samples are resistant to fibrinolysis (compared to plasma from controls and T2DM), even after trypsinisation. After a second trypsinization, the persistent pellet deposits (microclots) were solubilized. We detected various inflammatory molecules that are substantially increased in both the supernatant and trapped in the solubilized pellet deposits of acute COVID-19 and Long COVID/PASC, versus the equivalent volume of fully digested fluid of the control samples and T2DM. Of particular interest was a substantial increase in α(2)-antiplasmin (α2AP), various fibrinogen chains, as well as Serum Amyloid A (SAA) that were trapped in the solubilized fibrinolytic-resistant pellet deposits.
Conclusions
Clotting pathologies in both acute COVID-19 infection and in Long COVID/PASC might benefit from following a regime of continued anticlotting therapy to support the fibrinolytic system function.
[...]
cardiab.biomedcentral.com [2023-01-03] Etheresia Pretorius, Mare Vlok, ..., Douglas B. Kell, 23 August 2021 link archive General
Severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2)-induced infection, the cause of coronavirus disease 2019 (COVID-19), is characterized by unprecedented clinical pathologies. One of the most important pathologies, is hypercoagulation and microclots in the lungs of patients. Here we study the effect of isolated SARS-CoV-2 spike protein S1 subunit as potential inflammagen sui generis. Using scanning electron and fluorescence microscopy as well as mass spectrometry, we investigate the potential of this inflammagen to interact with platelets and fibrin(ogen) directly to cause blood hypercoagulation. Using platelet-poor plasma (PPP), we show that spike protein may interfere with blood flow. Mass spectrometry also showed that when spike protein S1 is added to healthy PPP, it results in structural changes to β and γ fibrin(ogen), complement 3, and prothrombin. These proteins were substantially resistant to trypsinization, in the presence of spike protein S1. Here we suggest that, in part, the presence of spike protein in circulation may contribute to the hypercoagulation in COVID-19 positive patients and may cause substantial impairment of fibrinolysis. Such lytic impairment may result in the persistent large microclots we have noted here and previously in plasma samples of COVID-19 patients. This observation may have important clinical relevance in the treatment of hypercoagulability in COVID-19 patients.
portlandpress.com [2023-01-03] Lize M. Grobbelaar, Chantelle Venter, ..., Etheresia Pretorius, AUGUST 20 2021 link archive General
Post-acute sequelae of COVID (PASC), usually referred to as ‘Long COVID’ (a phenotype of COVID-19), is a relatively frequent consequence of SARS-CoV-2 infection, in which symptoms such as breathlessness, fatigue, ‘brain fog’, tissue damage, inflammation, and coagulopathies (dysfunctions of the blood coagulation system) persist long after the initial infection. It bears similarities to other post-viral syndromes, and to myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Many regulatory health bodies still do not recognize this syndrome as a separate disease entity, and refer to it under the broad terminology of ‘COVID’, although its demographics are quite different from those of acute COVID-19. A few years ago, we discovered that fibrinogen in blood can clot into an anomalous ‘amyloid’ form of fibrin that (like other β-rich amyloids and prions) is relatively resistant to proteolysis (fibrinolysis). The result, as is strongly manifested in platelet-poor plasma (PPP) of individuals with Long COVID, is extensive fibrin amyloid microclots that can persist, can entrap other proteins, and that may lead to the production of various autoantibodies. These microclots are more-or-less easily measured in PPP with the stain thioflavin T and a simple fluorescence microscope. Although the symptoms of Long COVID are multifarious, we here argue that the ability of these fibrin amyloid microclots (fibrinaloids) to block up capillaries, and thus to limit the passage of red blood cells and hence O2 exchange, can actually underpin the majority of these symptoms. Consistent with this, in a preliminary report, it has been shown that suitable and closely monitored ‘triple’ anticoagulant therapy that leads to the removal of the microclots also removes the other symptoms. Fibrin amyloid microclots represent a novel and potentially important target for both the understanding and treatment of Long COVID and related disorders.
ncbi.nlm.nih.gov [2023-01-03] Douglas B. Kell, Gert Jacobus Laubscher, Etheresia Pretorius, February 2022 link archive General
SARS-CoV-2 infection is associated with a surprising number of morbidities. Uncanny similarities with amyloid-disease associated blood coagulation and fibrinolytic disturbances together with neurologic and cardiac problems led us to investigate the amyloidogenicity of the SARS-CoV-2 spike protein (S-protein). Amyloid fibril assays of peptide library mixtures and theoretical predictions identified seven amyloidogenic sequences within the S-protein. All seven peptides in isolation formed aggregates during incubation at 37 °C. Three 20-amino acid long synthetic spike peptides (sequence 192–211, 601–620, 1166–1185) fulfilled three amyloid fibril criteria: nucleation dependent polymerization kinetics by ThT, Congo red positivity, and ultrastructural fibrillar morphology. Full-length folded S-protein did not form amyloid fibrils, but amyloid-like fibrils with evident branching were formed during 24 h of S-protein coincubation with the protease neutrophil elastase (NE) in vitro. NE efficiently cleaved S-protein, rendering exposure of amyloidogenic segments and accumulation of the amyloidogenic peptide 194–203, part of the most amyloidogenic synthetic spike peptide. NE is overexpressed at inflamed sites of viral infection. Our data propose a molecular mechanism for potential amyloidogenesis of SARS-CoV-2 S-protein in humans facilitated by endoproteolysis. The prospective of S-protein amyloidogenesis in COVID-19 disease associated pathogenesis can be important in understanding the disease and long COVID-19.
pubs.acs.org [2023-01-03] Sofie Nyström, Per Hammarström, May 17, 2022 link archive General
Experimental findings for SARS-CoV-2 related to the glycan biochemistry of coronaviruses indicate that attachments from spike protein to glycoconjugates on the surfaces of red blood cells (RBCs), other blood cells and endothelial cells are key to the infectivity and morbidity of COVID-19. To provide further insight into these glycan attachments and their potential clinical relevance, the classic hemagglutination (HA) assay was applied using spike protein from the Wuhan, Alpha, Delta and Omicron B.1.1.529 lineages of SARS-CoV-2 mixed with human RBCs. The electrostatic potential of the central region of spike protein from these four lineages was studied through molecular modeling simulations. Inhibition of spike protein-induced HA was tested using the macrocyclic lactone ivermectin (IVM), which is indicated to bind strongly to SARS-CoV-2 spike protein glycan sites. The results of these experiments were, first, that spike protein from these four lineages of SARS-CoV-2 induced HA. Omicron induced HA at a significantly lower threshold concentration of spike protein than for the three prior lineages and was much more electropositive on its central spike protein region. IVM blocked HA when added to RBCs prior to spike protein and reversed HA when added afterwards. These results validate and extend prior findings on the role of glycan bindings of viral spike protein in COVID-19. They furthermore suggest therapeutic options using competitive glycan-binding agents such as IVM and may help elucidate rare serious adverse effects (AEs) associated with COVID-19 mRNA vaccines which use spike protein as the generated antigen.
The degree of myocardial injury, as reflected by troponin elevation, and associated outcomes among U.S. hospitalized patients with coronavirus disease-2019 (COVID-19) are unknown.
Objectives
The purpose of this study was to describe the degree of myocardial injury and associated outcomes in a large hospitalized cohort with laboratory-confirmed COVID-19.
Methods
Patients with COVID-19 admitted to 1 of 5 Mount Sinai Health Systemhospitals in New York City between February 27, 2020, and April 12, 2020, with troponin-I (normal value <0.03 ng/ml) measured within 24 h of admission were included (n = 2,736). Demographics, medical histories, admission laboratory results, and outcomes were captured from the hospitals’ electronic health records.
Results
The median age was 66.4 years, with 59.6% men. Cardiovascular disease (CVD), including coronary artery disease, atrial fibrillation, and heart failure, was more prevalent in patients with higher troponin concentrations, as were hypertension and diabetes. A total of 506 (18.5%) patients died during hospitalization. In all, 985 (36%) patients had elevated troponin concentrations. After adjusting for disease severity and relevant clinical factors, even small amounts of myocardial injury (e.g., troponin I >0.03 to 0.09 ng/ml; n = 455; 16.6%) were significantly associated with death (adjusted hazard ratio: 1.75; 95% CI: 1.37 to 2.24; p < 0.001) while greater amounts (e.g., troponin I >0.09 ng/dl; n = 530; 19.4%) were significantly associated with higher risk (adjusted HR: 3.03; 95% CI: 2.42 to 3.80; p < 0.001).
Conclusions
Myocardial injury is prevalent among patients hospitalized with COVID-19; however, troponin concentrations were generally present at low levels. Patients with CVD are more likely to have myocardial injury than patients without CVD. Troponin elevation among patients hospitalized with COVID-19 is associated with higher risk of mortality.
sciencedirect.com [2023-07-30] Anuradha Lala, Kipp W. Johnson, ..., Valentin Fuster, 4 August 2020 link archive General
Myocardial damage with a consequent rise in cardio-specific troponin level is a frequent phenomenon in severe cases of coronavirus disease 2019 (COVID-19). Its causes are capillary endothelial cell dysfunction, associated carditis, low oxygenization, and increased sympathetic tone, which all worsen myocardial stiffness and microvascular dysfunction (MD). They lead to severe myocardial dysfunction, arrhythmia, acute congestive heart failure, and a significant rise in death cases. During COVID-19, no specific cardiological treatment is started. As adjuvant therapy, anxiolytics in COVID-19 are widely used, but not in all anxious patients who had been infected with coronavirus. Anxiolytics can be useful to moderate MD and immunosuppressive effect of anxiety. The favorable effects of trimetazidine (TMZ) and Coenzyme Q10 (CoQ10) in the treatment of myocardial ischemia and heart failure had previously been proven, and also their anti-inflammatory effects had been suspected; however, they have not yet been used in COVID-19 cases. TMZ promotes glucose-mediated ATP production, which requires less oxygen, which explains its advantageous cardiac effects. Since it lowers serum and myocardial tissue proinflammatory cytokine levels and inhibits myocardial macrophage infiltration, it was suspected that TMZ might represent a novel therapeutic agent to prevent and treat sepsis-induced myocardial dysfunction. CoQ10 plays an important role in cellular ATP production; however, its concentration is decreased in cardiovascular diseases and in influenza patients. Due to its anti-inflammatory effect, CoQ10 has been suspected to have a key therapeutic target in influenza infection. We suggest considering these medicines to alleviate myocardial damage and inflammation in COVID-19.
pubmed.ncbi.nlm.nih.gov [2022-02-18] Mihály Medvegy, Gábor Simonyi, June, 2021 link archive General
Myocarditis and pericarditis are potential post-acute cardiac sequelae of COVID-19 infection, arising from adaptive immune responses. We aimed to study the incidence of post-acute COVID-19 myocarditis and pericarditis. Retrospective cohort study of 196,992 adults after COVID-19 infection in Clalit Health Services members in Israel between March 2020 and January 2021. Inpatient myocarditis and pericarditis diagnoses were retrieved from day 10 after positive PCR. Follow-up was censored on 28 February 2021, with minimum observation of 18 days. The control cohort of 590,976 adults with at least one negative PCR and no positive PCR were age- and sex-matched. Since the Israeli vaccination program was initiated on 20 December 2020, the time-period matching of the control cohort was calculated backward from 15 December 2020. Nine post-COVID-19 patients developed myocarditis (0.0046%), and eleven patients were diagnosed with pericarditis (0.0056%). In the control cohort, 27 patients had myocarditis (0.0046%) and 52 had pericarditis (0.0088%). Age (adjusted hazard ratio [aHR] 0.96, 95% confidence interval [CI]; 0.93 to 1.00) and male sex (aHR 4.42; 95% CI, 1.64 to 11.96) were associated with myocarditis. Male sex (aHR 1.93; 95% CI 1.09 to 3.41) and peripheral vascular disease (aHR 4.20; 95% CI 1.50 to 11.72) were associated with pericarditis. Post COVID-19 infection was not associated with either myocarditis (aHR 1.08; 95% CI 0.45 to 2.56) or pericarditis (aHR 0.53; 95% CI 0.25 to 1.13). We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.
mdpi.com [2022-07-09] Ortal Tuvali, Sagi Tshori, Estela Derazne, ..., Jacob George, 25 March 2022 link archive General
Question What is the prevalence of myocarditis in competitive athletes after COVID-19 infection, and how would different approaches to screening affect detection?
Findings In this cohort study of 1597 US competitive collegiate athletes undergoing comprehensive cardiovascular testing, the prevalence of clinical myocarditis based on a symptom-based screening strategy was only 0.31%. Screening with cardiovascular magnetic resonance imaging increased the prevalence of clinical and subclinical myocarditis by a factor of 7.4 to 2.3%.
Meaning These cardiac magnetic resonance imaging findings provide important data on the prevalence of clinical and subclinical myocarditis in college athletes recovering from symptomatic and asymptomatic COVID-19 infections.
Abstract
Importance Myocarditis is a leading cause of sudden death in competitive athletes. Myocardial inflammation is known to occur with SARS-CoV-2. Different screening approaches for detection of myocarditis have been reported. The Big Ten Conference requires comprehensive cardiac testing including cardiac magnetic resonance (CMR) imaging for all athletes with COVID-19, allowing comparison of screening approaches.
Objective To determine the prevalence of myocarditis in athletes with COVID-19 and compare screening strategies for safe return to play.
Design, Setting, and Participants Big Ten COVID-19 Cardiac Registry principal investigators were surveyed for aggregate observational data from March 1, 2020, through December 15, 2020, on athletes with COVID-19. For athletes with myocarditis, presence of cardiac symptoms and details of cardiac testing were recorded. Myocarditis was categorized as clinical or subclinical based on the presence of cardiac symptoms and CMR findings. Subclinical myocarditis classified as probable or possible myocarditis based on other testing abnormalities. Myocarditis prevalence across universities was determined. The utility of different screening strategies was evaluated.
Exposures SARS-CoV-2 by polymerase chain reaction testing.
Main Outcome and Measure Myocarditis via cardiovascular diagnostic testing.
Results Representing 13 universities, cardiovascular testing was performed in 1597 athletes (964 men [60.4%]). Thirty-seven (including 27 men) were diagnosed with COVID-19 myocarditis (overall 2.3%; range per program, 0%-7.6%); 9 had clinical myocarditis and 28 had subclinical myocarditis. If cardiac testing was based on cardiac symptoms alone, only 5 athletes would have been detected (detected prevalence, 0.31%). Cardiac magnetic resonance imaging for all athletes yielded a 7.4-fold increase in detection of myocarditis (clinical and subclinical). Follow-up CMR imaging performed in 27 (73.0%) demonstrated resolution of T2 elevation in all (100%) and late gadolinium enhancement in 11 (40.7%).
Conclusions and Relevance In this cohort study of 1597 US competitive athletes with CMR screening after COVID-19 infection, 37 athletes (2.3%) were diagnosed with clinical and subclinical myocarditis. Variability was observed in prevalence across universities, and testing protocols were closely tied to the detection of myocarditis. Variable ascertainment and unknown implications of CMR findings underscore the need for standardized timing and interpretation of cardiac testing. These unique CMR imaging data provide a more complete understanding of the prevalence of clinical and subclinical myocarditis in college athletes after COVID-19 infection. The role of CMR in routine screening for athletes safe return to play should be explored further.
Participants were recruited from COVIDsortium, a 3-hospital prospective study of 731 health care workers who underwent first-wave weekly symptom, polymerase chain reaction, and serology assessment over 4 months, with seroconversion in 21.5% (n = 157). At 6 months post-infection, 74 seropositive and 75 age-, sex-, and ethnicity-matched seronegative control subjects were recruited for cardiovascular phenotyping (comprehensive phantom-calibrated cardiovascular magnetic resonance and blood biomarkers). Analysis was blinded, using objective artificial intelligence analytics where available.
Results
A total of 149 subjects (mean age 37 years, range 18 to 63 years, 58% women) were recruited. Seropositive infections had been mild with case definition, noncase definition, and asymptomatic disease in 45 (61%), 18 (24%), and 11 (15%), respectively, with 1 person hospitalized (for 2 days). Between seropositive and seronegative groups, there were no differences in cardiac structure (left ventricular volumes, mass, atrial area), function (ejection fraction, global longitudinal shortening, aortic distensibility), tissue characterization (T1, T2, extracellular volume fraction mapping, late gadolinium enhancement) or biomarkers (troponin, N-terminal pro–B-type natriuretic peptide). With abnormal defined by the 75 seronegatives (2 SDs from mean, e.g., ejection fraction <54%, septal T1 >1,072 ms, septal T2 >52.4 ms), individuals had abnormalities including reduced ejection fraction (n = 2, minimum 50%), T1 elevation (n = 6), T2 elevation (n = 9), late gadolinium enhancement (n = 13, median 1%, max 5% of myocardium), biomarker elevation (borderline troponin elevation in 4; all N-terminal pro–B-type natriuretic peptide normal). These were distributed equally between seropositive and seronegative individuals.
Conclusions
Cardiovascular abnormalities are no more common in seropositive versus seronegative otherwise healthy, workforce representative individuals 6 months post–mild severe acute respiratory syndrome-coronavirus-2 infection.
sciencedirect.com [2022-11-23] George Joy, Jessica Artico, James C. Moon, November 2021 link archive General
Myocarditis and pericarditis are potential post-acute cardiac sequelae of COVID-19 infection, arising from adaptive immune responses. We aimed to study the incidence of post-acute COVID-19 myocarditis and pericarditis. Retrospective cohort study of 196,992 adults after COVID-19 infection in Clalit Health Services members in Israel between March 2020 and January 2021. Inpatient myocarditis and pericarditis diagnoses were retrieved from day 10 after positive PCR. Follow-up was censored on 28 February 2021, with minimum observation of 18 days. The control cohort of 590,976 adults with at least one negative PCR and no positive PCR were age- and sex-matched. Since the Israeli vaccination program was initiated on 20 December 2020, the time-period matching of the control cohort was calculated backward from 15 December 2020. Nine post-COVID-19 patients developed myocarditis (0.0046%), and eleven patients were diagnosed with pericarditis (0.0056%). In the control cohort, 27 patients had myocarditis (0.0046%) and 52 had pericarditis (0.0088%). Age (adjusted hazard ratio [aHR] 0.96, 95% confidence interval [CI]; 0.93 to 1.00) and male sex (aHR 4.42; 95% CI, 1.64 to 11.96) were associated with myocarditis. Male sex (aHR 1.93; 95% CI 1.09 to 3.41) and peripheral vascular disease (aHR 4.20; 95% CI 1.50 to 11.72) were associated with pericarditis. Post COVID-19 infection was not associated with either myocarditis (aHR 1.08; 95% CI 0.45 to 2.56) or pericarditis (aHR 0.53; 95% CI 0.25 to 1.13). We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.
mdpi.com [2022-11-23] Ortal Tuvali, Sagi Tshori, ..., Jacob George, 15 April 2022 link archive General
The COVID-19 pandemic, the result of severe acute respiratory syndrome (SARS)-CoV-2, is a major cause of worldwide mortality with a significant cardiovascular component. While a number of different cardiovascular histopathologies have been reported at postmortem examination, their incidence is unknown, due to limited numbers of cases in any given study. A literature review was performed identifying 277 autopsied hearts across 22 separate publications of COVID-19 positive patients. The median age of the autopsy cohort was 75 and 97.6% had one or more comorbidities. Initial review of the data indicate that myocarditis was present in 20 hearts (7.2%); however, closer examination of additional reported information revealed that most cases were likely not functionally significant and the true prevalence of myocarditis is likely much lower (<2%). At least one acute, potentially COVID-19-related cardiovascular histopathologic finding, such as macro or microvascular thrombi, inflammation, or intraluminal megakaryocytes, was reported in 47.8% of cases. Significant differences in reporting of histopathologic findings occurred between studies indicating strong biases in observations and the need for more consistency in reporting. In conclusion, across 277 cases, COVID-19-related cardiac histopathological findings, are common, while myocarditis is rare.
This was a key study that was sidelined. The reality today is post-COVID vaccine, we are seeing substantial myocarditis (vaccine induced and linked) yet we have evidence such as this study below telling us that myocarditis was seldom found in COVID-19 autopsies, where the deceased person had no vaccine, yet had prior COVID-19 infection (looking here at autopsied hearts across 22 separate publications of COVID-19 positive patients).
pubmed.ncbi.nlm.nih.gov [2022-12-20] Marc K Halushka, Richard S Vander Heide, link archive General
Association between messenger RNA (mRNA) COVID-19 vaccines and myocarditis has aroused public concern over vaccine safety.
Objectives
The goal of this study was to compare the prognosis of this condition with viral infection–related myocarditis over 180 days.
Methods
A territory-wide electronic public health care database in Hong Kong linked with population-based vaccination records was used to conduct a retrospective cohort study. Since the roll-out of BNT162b2 (Pfizer-BioNTech), patients aged ≥12 years hospitalized with myocarditis within 28 days after BNT162b2 vaccination were compared against viral infection–related myocarditis recorded before the pandemic (2000-2019), over a 180-day follow-up period (starting from diagnosis of myocarditis). All-cause mortality, heart failure, dilated cardiomyopathy, heart transplant, and postdischarge health care utilization were examined with Cox proportional hazards models.
Results
A total of 866 patients were included for analysis. Over the follow-up period, 1 death (1.0%) of 104 patients with postvaccination myocarditis and 84 deaths (11.0%) of 762 patients with viral infection–related myocarditis were identified. One case (1.0%) of dilated cardiomyopathy and 2 cases (1.9%) of heart failure were identified in the postvaccination group, compared with 28 (3.7%) and 93 (12.2%) in the viral infection–related myocarditis group, respectively. Adjusted analysis showed that the postvaccination myocarditis group had a 92% lower mortality risk (adjusted HR: 0.08; 95% CI: 0.01-0.57). No significant differences in other prognostic outcomes were seen.
Conclusions
This study found a significantly lower rate of mortality among individuals with myocarditis after mRNA vaccination compared with those with viral infection–related myocarditis. Prognosis of this iatrogenic condition may be less severe than naturally acquired viral infection–related myocarditis.
The natural history of vaccine-induced myocarditis for outcomes such as heart failure, dilated cardiomyopathy, or death is far different—more favorable—than from Covid myocarditis (besides the latter being considerably more common) https://t.co/2de1Eth12Npic.twitter.com/UKOMRKYNt0
And so, it is neither surprising nor reassuring that extreme outcomes like death are so frequent in the highly co-morbid post-viral group, but rare in the previously healthy post-BNT162b2 group, in the incredibly brief time-frame being measured.
[...]
By post-infection myocarditis being “considerably more common,” Eric Topol presumably means “if you consider only all people together, old and young, and stonewall the clear and repeated findings of higher rates in young males forever” (repeat a lie often enough, as they say).
sciencedirect.com [2022-12-23] Francisco Tsz Tsun Lai, Edward Wai Wa Chan, Lei Huang, ..., Ian Chi Kei Wong, 13 December 2022 link archive General
Background: The COVID-19 (coronavirus disease 2019) pandemic is reducing health care accessibility to non–life-threatening diseases, thus hiding their real incidence. Moreover, the incidence of potentially fatal conditions such as acute type A aortic dissection seems to have decreased since the pandemic began, whereas the number of cases of chronic ascending aortic dissections dramatically increased. We present two patients whose management has been affected by the exceptional sanitary situation we are dealing with.
Case report: A 70-year-old man with chest pain and an aortic regurgitation murmur had his cardiac workup delayed (4 months) because of sanitary restrictions. He was then diagnosed with chronic type A aortic dissection and underwent urgent replacement of ascending aorta and aortic root. The delay in surgical treatment made the intervention technically challenging because the ascending aorta grew up to 80 mm inducing strong adhesions and chronic inflammation. The second case report concerns a 68-year-old woman with right lower-limb pain who was diagnosed with deep vein thrombosis. However, a CT scan to exclude a pulmonary embolism could not be realized until 5 months later because of sanitary restrictions. When she eventually got the CT scan, it fortuitously showed a chronic dissection of the ascending aorta. She underwent urgent surgery, and the intervention was challenging because of adhesions and severe inflammation.
Conclusion: Delayed treatment due to sanitary restrictions related to COVID-19 pandemic is having a significant impact on the management of potentially life-threatening conditions including type A aortic dissection. We should remain careful to avoid COVID-19 also hitting patients who are not infected with the virus.
frontiersin.org [2023-01-14] Arnaud Lyon, Ziyad Gunga, Lars Niclauss, Valentina Rancati, Piergiorgio Tozzi, 28 April 2021 link archive General
Coronavirus disease 19 (Covid-19) has been declared as a pandemic disease since March 2020; causing wide array of signs and symptoms, many of which result in increased mortality rates worldwide. Although it was initially known as an acute respiratory disease, Covid-19 is accompanied with several extrapulmonary manifestations, of which the cardiovascular ones are of major importance. Among other cardiovascular complications of Covid-19, aortic dissection has been a significant yet underrated problem. The pathophysiology of aortic dissection consists of various inflammatory pathways, that could be influenced by Covid-19 infection. We herein have reviewed articles inclusive of aortic dissection concurrent with Covid-19 infection in a systematic manner, along with the probable similarities in pathophysiology of aortic dissection with Covid-19 infection.
ncbi.nlm.nih.gov [2023-01-14] Alireza Ramandi, Mohammad Ali Akbarzadeh, Isa Khaheshi, Mohammad Reza Khalilian, February 2022 link archive General
Myocarditis and pericarditis are potential post-acute cardiac sequelae of COVID-19 infection, arising from adaptive immune responses. We aimed to study the incidence of post-acute COVID-19 myocarditis and pericarditis. Retrospective cohort study of 196,992 adults after COVID-19 infection in Clalit Health Services members in Israel between March 2020 and January 2021. Inpatient myocarditis and pericarditis diagnoses were retrieved from day 10 after positive PCR. Follow-up was censored on 28 February 2021, with minimum observation of 18 days. The control cohort of 590,976 adults with at least one negative PCR and no positive PCR were age- and sex-matched. Since the Israeli vaccination program was initiated on 20 December 2020, the time-period matching of the control cohort was calculated backward from 15 December 2020. Nine post-COVID-19 patients developed myocarditis (0.0046%), and eleven patients were diagnosed with pericarditis (0.0056%). In the control cohort, 27 patients had myocarditis (0.0046%) and 52 had pericarditis (0.0088%). Age (adjusted hazard ratio [aHR] 0.96, 95% confidence interval [CI]; 0.93 to 1.00) and male sex (aHR 4.42; 95% CI, 1.64 to 11.96) were associated with myocarditis. Male sex (aHR 1.93; 95% CI 1.09 to 3.41) and peripheral vascular disease (aHR 4.20; 95% CI 1.50 to 11.72) were associated with pericarditis. Post COVID-19 infection was not associated with either myocarditis (aHR 1.08; 95% CI 0.45 to 2.56) or pericarditis (aHR 0.53; 95% CI 0.25 to 1.13). We did not observe an increased incidence of neither pericarditis nor myocarditis in adult patients recovering from COVID-19 infection.
pubmed.ncbi.nlm.nih.gov [2023-03-29] Ortal Tuvali, Sagi Tshori, ..., Jacob George, April 2022 link archive General
Background: Many postmortem studies address the cardiovascular effects of COVID-19 and provide valuable information, but are limited by their small sample size.
Objectives: The aim of this systematic review is to better understand the various aspects of the cardiovascular complications of COVID-19 by pooling data from a large number of autopsy studies.
[...]
Results: This review cohort contained 50 studies including 548 hearts. The median age of the deceased was 69 years. The most prevalent acute cardiovascular findings were myocardial necrosis (median: 100.0%; IQR, 20%-100%; number of studies = 9; number of patients = 64) and myocardial oedema (median: 55.5%; IQR, 19.5%-92.5%; number of studies = 4; number of patients = 46). The median reported prevalence of extensive, focal active, and multifocal myocarditis were all 0.0%. The most prevalent chronic changes were myocyte hypertrophy (median: 69.0%; IQR, 46.8%-92.1%) and fibrosis (median: 35.0%; IQR, 35.0%-90.5%). SARS-CoV-2 was detected in the myocardium with median prevalence of 60.8% (IQR 40.4-95.6%).
Conclusions: Our systematic review confirmed the high prevalence of acute and chronic cardiac pathologies in COVID-19 and SARS-CoV-2 cardiac tropism, as well as the low prevalence of myocarditis in COVID-19.
In summary, this review should be the nail in the coffin in ruling out COVID-19 illness as a cause of fatal myocarditis. Despite the virus being found in heart tissue, it was not causing significant inflammation. The explosion of fatal myocarditis by report of unexplained cardiac arrest, adjudication, and at necropsy must have another explanation than SARS-CoV-2 infection. The only new proven cause of heart damage in human populations is COVID-19 vaccination. Vaccines used in America (Pfizer, Moderna, Janssen, Novavax) have been demonstrated to cause myocarditis as published in the peer-reviewed literature.
pubmed.ncbi.nlm.nih.gov [2023-03-29] Raghed Almamlouk, Tarek Kashour, ..., Zachary Grimes, March 2023 link archive General
Persistent SARS-CoV-2 infection model of human cardiac tissue was established
Hypoxic stress to the persistent infection model led to cardiac dysfunction
ACE2 and SARS-CoV-2 S protein expression were elevated after the hypoxic stress
This research may predict a “heart failure pandemic” in the post COVID-19 era
Summary
Patients with chronic cardiomyopathy may have persistent viral infections in their hearts, particularly with SARS-CoV-2, which targets the ACE2 receptor highly expressed in human hearts. This raises concerns about a potential global heart failure pandemic stemming from COVID-19, an SARS-CoV-2 pandemic in near future. Although faced with this healthcare caveat, there is limited research on persistent viral heart infections, and no models have been established. In this study, we created an SARS-CoV-2 persistent infection model using human iPS cell-derived cardiac microtissues (CMTs). Mild infections sustained viral presence without significant dysfunction for a month, indicating persistent infection. However, when exposed to hypoxic conditions mimicking ischemic heart diseases, cardiac function deteriorated alongside intracellular SARS-CoV-2 reactivation in cardiomyocytes and disrupted vascular network formation. This study demonstrates that SARS-CoV-2 persistently infects the heart opportunistically causing cardiac dysfunction triggered by detrimental stimuli such as ischemia, potentially predicting a post COVID-19 era heart failure pandemic.
The researchers begin with the Covidian theory of persistent covid infection — a stealthiest kind of crypto-covid infection ever, which is not only asymptomatic but also tests negative, even using PCR — which has been criticized for being too sensitive. In fact, persistent covid is completely invisible to testing. So far.
So, it’s kind of a religious belief.
Notably, the researchers predicted a pandemic of heart failure which, they say, will be evidenced by finding spike protein in cardiac tissue. Even though they admitted there’s no conclusive evidence for persistent covid infection so far, they feel the alarm bells should already be going off about heart attacks:
The explosive increase in the number of virus-infected patients due to the COVID-19 pandemic may have led to an enormous increase in the number of patients at potential risk for future heart failure. In clinical practices, such high-risk patients should be identified by detecting the virus itself or the viral genome in endocardial biopsy tissue or by monitoring blood troponin levels. This report may serve as a warning for the possibility of a heart failure pandemic in the post COVID-19 era.
The study does not, and wasn’t intended to, show persistent covid infection. The researchers infected some cardiac cells with covid in a Petri dish and looked to see what happens. Since there’s no immune system in a Petri dish, it couldn’t show viral persistence in the body. But it did show what happens to cardiac cells when spike protein gets into them through viral infection or mRNA transfection. Which is: nothing good.
I thought the author’s illustration (above) sort of gave away what they’re really thinking about. The upper panel at the far left shows increasing spike protein not virus. Only one thing causes spike without virus: the jabs.
“Persistent covid” — which sounds a lot more scientific than “long covid” — would sure be a good cover for jab injuries, if they can find some evidence for it somewhere.
sciencedirect.com [2023-12-29] Kozue Murata, Akiko Makino, Keizo Tomonaga, Hidetoshi Masumoto, 22 December 2023 link archive General
Wow. Scientists are now warning that the latest COVID variant could trigger a “heart failure pandemic.”
And get this: Pfizer, the same company that sold you the so-called vaccines, is making a big bet on that “heart failure pandemic.”
The pharmaceutical giant recently acquired several companies. This includes a major $6.7 billion cash acquisition of Arena Pharmaceuticals, a firm specializing in developing treatments, particularly for heart inflammation conditions like myocarditis and pericarditis.
So, the company that caused the heart damage is now looking to profit from heart damage. Is my analysis wrong here?
Fischer et al evaluated 587 consecutive patients with suspected, pre-pandemic myocarditis who underwent CMR and ECG for 15 years. They followed patients for major adverse cardiovascular event (MACE) included all-cause death, hospitalization for heart failure, heart transplantation, documented sustained ventricular arrhythmia, or recurrent myocarditis.
Both the ECG and cardiac MRI results where prognostic for the composite outcome. Conversely, those with normal ECG and MRI findings had the lowest rates of cardiac events over 15 years. The importance of this study for our patients with COVID-19 vaccine myocarditis is that each patient and their family should know and keep their initial and follow-up ECG and MRI results. Hopefully normalization will confer the best overall outlook. Conversely, those with abnormal findings should have continued close follow-up.
SARS-CoV-2 can cause acute respiratory distress and death in some patients1. Although severe COVID-19 is linked to substantial inflammation, how SARS-CoV-2 triggers inflammation is not clear2. Monocytes and macrophages are sentinel cells that sense invasive infection to form inflammasomes that activate caspase-1 and gasdermin D, leading to inflammatory death (pyroptosis) and the release of potent inflammatory mediators3. Here we show that about 6% of blood monocytes of patients with COVID-19 are infected with SARS-CoV-2. Monocyte infection depends on the uptake of antibody-opsonized virus by Fcγ receptors. The plasma of vaccine recipients does not promote antibody-dependent monocyte infection. SARS-CoV-2 begins to replicate in monocytes, but infection is aborted, and infectious virus is not detected in the supernatants of cultures of infected monocytes. Instead, infected cells undergo pyroptosis mediated by activation of NLRP3 and AIM2 inflammasomes, caspase-1 and gasdermin D. Moreover, tissue-resident macrophages, but not infected epithelial and endothelial cells, from lung autopsies from patients with COVID-19 have activated inflammasomes. Taken together, these findings suggest that antibody-mediated SARS-CoV-2 uptake by monocytes and macrophages triggers inflammatory cell death that aborts the production of infectious virus but causes systemic inflammation that contributes to COVID-19 pathogenesis.
[...]
nature.com [2022-12-13] Caroline Junqueira, Ângela Crespo, ..., Jonathan Abraham, ..., Judy Lieberman, 06 April 2022 link archive General
Molecular mimicry between viral antigens and host proteins can produce cross-reacting antibodies leading to autoimmunity. The coronavirus SARS-CoV-2 causes COVID-19, a disease curiously resulting in varied symptoms and outcomes, ranging from asymptomatic to fatal. Autoimmunity due to cross-reacting antibodies resulting from molecular mimicry between viral antigens and host proteins may provide an explanation. Thus, we computationally investigated molecular mimicry between SARS-CoV-2 Spike and known epitopes. We discovered molecular mimicry hotspots in Spike and highlight two examples with tentative high autoimmune potential and implications for understanding COVID-19 complications. We show that a TQLPP motif in Spike and thrombopoietin shares similar antibody binding properties. Antibodies cross-reacting with thrombopoietin may induce thrombocytopenia, a condition observed in COVID-19 patients. Another motif, ELDKY, is shared in multiple human proteins, such as PRKG1 involved in platelet activation and calcium regulation, and tropomyosin, which is linked to cardiac disease. Antibodies cross-reacting with PRKG1 and tropomyosin may cause known COVID-19 complications such as blood-clotting disorders and cardiac disease, respectively. Our findings illuminate COVID-19 pathogenesis and highlight the importance of considering autoimmune potential when developing therapeutic interventions to reduce adverse reactions.
mdpi.com [2022-11-23] Janelle Nunez-Castilla, Vitalii Stebliankin, ..., Kalai Mathee, Jessica Siltberg-Liberles, link archive General
Ly49+CD8+ T cells are a subset of CD8+ T cells that show immunoregulatory activity in mice. Li et al. report the existence of a similar CD8+ T cell subset in humans that expresses killer cell immunoglobulin-like receptors (KIRs), a functional parallel of the mouse Ly49 family (see the Perspective by Levescot and Bensussan). These cells, which can suppress self-reactive CD4+ T cells, were more abundant in patients with autoimmune conditions such as celiac disease, multiple sclerosis, and lupus, as well as in patients infected with influenza virus or severe acute respiratory syndrome coronavirus 2. When mice selectively deficient in Ly49+CD8+ T cells were infected with viruses, they showed normal antiviral immune responses but eventually developed symptoms of autoimmune disease. KIR+CD8+ T cells may therefore be an important therapeutic target for the control of autoimmune diseases such as “long COVID” that emerge after viral infections. —STS
Structured Abstract
INTRODUCTION
Previous studies have identified Ly49+CD8+ T cells as a CD8+ T cell subset with regulatory functions in mice. These cells can suppress myelin oligodendrocyte glycoprotein (MOG)–specific pathogenic CD4+ T cells through their cytolytic activity and thereby ameliorate experimental autoimmune encephalomyelitis (EAE). However, whether a similar CD8+ regulatory T cell subset exists in humans and whether its suppressive activity extends beyond autoimmune diseases to play a more general role in peripheral tolerance remains to be determined.
[...]
CONCLUSION
We identify KIR+CD8+ T cells as an important regulatory T cell subset in humans. They are induced as part of the response during an autoimmune reaction or infection and may act as a negative feedback mechanism to specifically suppress the self-reactive or otherwise pathogenic cells without affecting the immune responses against pathogens. This subset of CD8+ Tregs appears to play an important role in maintaining peripheral tolerance, which is distinct from and likely complementary to that of CD4+ Tregs. Our findings also provide insights into understanding the relationship between autoimmunity and infectious diseases and into the development of potential therapeutic approaches targeting KIR+CD8+ T cells to suppress undesirable self-reactivity in autoimmune disorders and infectious diseases.
The increasing number of reports of mild to severe psychological, behavioral, and cognitive sequelae in COVID-19 survivors motivates a need for a thorough assessment of the neurological effects of the disease. In this regard, we have conducted a neuroimaging study to understand the neurotropic behavior of the coronavirus. We hypothesize that the COVID recovered subjects have developed alterations in the brain which can be measured through susceptibility differences in various regions of brain when compared to healthy controls (HCs). Hence we performed our investigations on susceptibility weighted imaging (SWI) volumes. Fatigue, being of the most common symptoms of Long COVID has also been studied in this work. SWI volumes of 46 COVID and 30 HCs were included in this study. The COVID patients were imaged within six months of their recovery. We performed unpaired two-sample t-test over the pre-processed SWI volumes of both the groups and multiple linear regression was performed to observe group differences and correlation of fatigue with SWI values. The group analysis showed that COVID recovered subjects had significantly higher susceptibility imaging values in regions of the frontal lobe and the brain stem. The clusters obtained in the frontal lobe primarily show differences in the white matter regions. The COVID group also demonstrated significantly higher fatigue levels than the HC group. The regression analysis on the COVID group yielded clusters in anterior cingulate gyrus and midbrain which exhibited negative correlations with fatigue scores. This study suggests an association of Long COVID with prolonged effects on the brain and also indicates the viability of SWI modality for analysis of post-COVID symptoms.
This study suggests association of Long COVID with prolonged effects on the brain & also indicates the viability of SWI modality for analysis of post-COVID symptoms; long COVID is real! spike damage
medrxiv.org [2022-12-06] Sapna S Mishra, Rakibul Hafiz, ..., Bharat B. Biswal, November 22, 2022 link archive General
New research to be presented at this year’s European Congress of Clinical Microbiology and Infectious Diseases (ECCMID 2022, Lisbon, 23-26 April) suggests that many of the symptoms connected to post-COVID syndrome (PCC, also known as long COVID) could be linked to the effect of the virus on the vagus nerve – one of the most important multi-functional nerves in the body. The study is by Dr Gemma Lladós and Dr Lourdes Mateu, University Hospital Germans Trias i Pujol, Badalona, Spain, and colleagues.
The vagus nerve extends from the brain down into the torso and into the heart, lungs and intestines, as well as several muscles including those involved in swallowing. As such, this nerve is responsible for a wide variety of bodily functions including controlling heart rate, speech, the gag reflex, transferring food from the mouth to the stomach, moving food through the intestines, sweating, and many others.
Multisystem inflammatory syndrome in children (MIS-C) is a rare but serious condition typically occurring 2–6 weeks after SARS-CoV-2 infection and characterized by fever and multiorgan involvement.
What is added by this report?
MIS-C incidence has decreased from early in the COVID-19 pandemic (highest in late 2020–early 2021), but cases continue to occur with a recent relative increase in the fall of 2023 after a period of increased COVID-19 activity in the general population. Among 117 patients with MIS-C in 2023, approximately one half required intensive care unit–level care. More than 80% (92 of 112) of MIS-C cases were in vaccine-eligible but unvaccinated children, and among the 20 vaccinated children, 60% likely had waned immunity at the time of MIS-C illness.
What are the implications for public health practice?
MIS-C cases continue to occur but at low rates, making ongoing surveillance valuable. COVID-19 vaccination remains important for preventing MIS-C.
[...]
Multisystem inflammatory syndrome in children (MIS-C) is a rare but serious condition typically occurring 2–6 weeks after SARS-CoV-2 infection and characterized by fever and multiorgan involvement (1,2). In May 2020, CDC created an MIS-C case definition and established a passive national surveillance system for voluntary case reporting by state and local health departments.* In 2022, CDC and the Council of State and Territorial Epidemiologists (CSTE) created a new surveillance case definition that went into effect on January 1, 2023† (3). Approximately 87% of cases reported using the 2020 case definition also meet the 2023 case definition. This report describes 2023 MIS-C cases and compares them with cases reported earlier in the COVID-19 pandemic.
Cases of multisystem inflammatory syndrome (MIS-C), a rare but serious COVID-19 complication in children, have decreased from the earlier pandemic months but continue to be reported, the Centers for Disease Control and Prevention (CDC) reported today in Morbidity and Mortality Weekly Report (MMWR).
You can see by the chart that after May 21, 2022, the cases of MIS-C were way down relative to COVID cases.
But the vaccine rolled out for 7-year-olds (the most vulnerable group for MIS-C in 2023 according to the CDC report) in May 2021, one year earlier.
So did the vaccine magically suddenly start working 1 year later?
Nope. The CDC paper says the protective effect of the vaccine wears off after a year.
The data shows that immunity started to rapidly happen starting March 1, 2022 when the orange curve started to break away from the blue bars in the plot above.
June 8, 1973, 10:30 AM, Ambassador Porter’s Office, State Department
COPIES TO: S, D, P, E, M, C, S/PC, S/S, EUR, IO, S/PM, AID
General Draper and his colleagues presented their views that the population explosion in developing countries was not only a threat to US interests in the economics and in the development of those countries but also, more fundamentally, presented a danger to our politico military interests. They referred to the memorandum written by General Taylor on this subject. Ambassador Porter said that he had read General Taylor’s memorandum and asked him to comment on it further if he cared to. General Taylor said he would add only that, although he was a neophyte in population matters, he felt very strongly that, as stated in his memorandum, the rapid growth of populations in many developing countries was a likely source of internal violence and of possibilities of external aggression. He and General Draper asked Ambassador Porter for his advice on how to proceed with the subject. They said they had talked to General Scowcroft in Mr. Kissinger’s office about it in terms of the possibility of a NSC study. General Draper said he had written the President explaining his views that rapid population growth could endanger the concept of a generation of peace and recommending that the President speak out on this subject.
[...]
Kissinger Report and Subsequent US Population Control Policy
The classified National Security Study Memo known as The Kissinger Report, undertaken at the direction of President Nixon, laid out detailed plans for population reduction in many countries. These plans became official US policy in 1975 though National Security Decision 314, enacted by President Gerald Ford.
The policies developed from the report were seen as a way the United States could use human population control to prevent undeveloped nations from gaining substantial political power. Believing that future generations birthed throughout the world posed a danger to wealth accumulation, the policy was backed by wealthy individuals in the US. The policy was also expected to protect American businesses abroad against interference from nations seeking to support their growing populations.
Historically, war was required to reduce an adversary’s population; the Kissinger Report proposed a more strategic and well-disguised approach aimed at countries that could pose long-term risk to U.S. economic and military interests.
From Wikipedia: “NSSM200 was reworked and adopted as official United States policy through NSDM 314 by President Gerald Ford on November 26, 1975. It was initially classified for over a decade but was obtained by researchers in the early 1990s. The memorandum and subsequent policies developed from the report were observed as a way the United States could use human population reduction to limit the political power of undeveloped nations, ensure the easy extraction of foreign natural resources, prevent young anti-establishment individuals from being born, and to protect American businesses abroad from interference from nations seeking to support their growing populations.”
From the Kissinger Report Executive Summary:
World policy and programs in the population field should incorporate two major objectives:
(a) actions to accommodate continued population growth up to 6 billions by the mid-21st century without massive starvation or total frustration of developmental hopes; and
(b) actions to keep the ultimate level as close as possible to 8 billions rather than permitting it to reach 10 billions, 13 billions, or more
This major objective –to not exceed 8-billion– combined with the fact that we hit the 8-billion mark in 2022 might help explain the intense urgency of so many planned and organized actions during the past three years.
When we set aside Covid/virus/pandemic (the ostensible rationale for everything that’s been done since 2020), and focus instead on plans that were developed and enacted by USG over decades, and when we focus on actions that have been taken on those plans, and when we focus on the effects that have been caused by those actions, it emerges that population reduction, population control (and control of the population) has resulted. This is expressed without judgement about good or bad motives, and without reference to specific people – simply looking at what has resulted.
[...]
The report recommends population control only in Least Developed Countries (LDC), and cautions that “We must take care that our activities should not give the appearance to the LDCs of an industrialized country policy directed against the LDCs,” though the policy was precisely that.
The report stresses more than once that weaving the concepts of family planning into health programs is a strategy for gaining acceptance, and will:
[...]
“Should the U.S. seek to change its own food consumption patterns toward more efficient uses of protein?”
Note: During the COVID pandemic, the FDA began a $5-billion program related to this, and the Gates Foundation has funded several projects along these lines. (While these pursuits are certainly not all bad, they are science-fiction projects that will change the natural food supply, and it might be too much to expect they will great care.)
The report proposes the commercial approach in which USG uses “big-medical research to improve the existing means of fertility control and to develop new ones.” (Note that this project was a National Security Directive, not inspired to to improve reproductive freedom – quite the opposite. There is no reproductive freedom when one can’t have children.)
The report favors “large-scale programs that will induce fertility decline in a cost-effective manner,” and enthusiastically describes controversial examples, such as what it calls “the remarkably successful experiments in India in which financial incentives, along with other motivational devices, were used to get large numbers of men to accept vasectomies.”
“Only a concerted and major effort in a number of carefully selected directions can provide the hope of success in reducing population growth...”
[...]
Main observations advanced by NSSM200:
Population growth of foreign nations provides more geopolitical power and possible opposition to US interests
The United States relies on countries being underdeveloped in order to easily obtain natural resources
American businesses are vulnerable to interference by foreign governments that are required to provide for growing populations
High birth rates result in more young individuals who oppose established governments
“Young people, who are in much higher proportions in many LDCs, are likely to be more volatile, unstable, prone to extremes, alienation and violence than an older population. These young people can more readily be persuaded to attack the legal institutions of the government or real property of the establishment, imperialists, multinational corporations, or other, often foreign [meaning U.S.] influences that are blamed for their troubles.”
[...]
From NSSM 200 and National Security Decision 314:
“The U.S. economy will require large and increasing amounts of minerals from abroad, especially from less developed countries.”
“In these sensitive relations, however, it is important in style as well as substance to avoid the appearance of coercion.”
“No country has reduced its population growth without resorting to abortion...”
The National Security Council recommended that world-wide support for population reduction should be sought through “increased emphasis on mass media and other population education and motivation programs by the UN, USIA, and USAID.”
The policies adopted from NSSM200 and NSDM 314 expanded even further in 1976 after the National Security Council advocated for the use of withholding food as a strategy of influence (food power), and using military force to prevent population growth.
“In some cases, strong direction has involved incentives such as payment to acceptors for sterilization, or disincentives such as giving low priorities in the allocation of housing or schooling to those with larger families. Such direction is the sine qua non of an effective program.”
[...]
Top 10
Here are the top 10 methods “they” are using to reduce human population down to a “manageable” amount, at which point those remaining (apparently including the heirs to the fortunes of those driving this bus) will all live in a “utopian society”. Personally, I suspect that the result will be more akin to the dystopia of “Mad Max” than enlightened Athenian Democracy or Platos Republic.
Method 10: Targeted sterilization
Throughout history, and still today, people have used the philosophy of Eugenics to “improve” the human population by deciding who shouldn’t be allowed to have children. Oftentimes this means sterilizing the Sick and/or Poor.
Admitted cases of targeted sterilization include some 33 States of the United States from the 1930’s-1980’s. In the case of North Carolina they even apologized and established the N.C. Justice for Sterilization Victims Foundation in 2010 to compensate victims.
Other cases of forced sterilization include Nazi Germany and rumored immunization vaccines laced with antibodies to render woman sterile in the Philippines and in Africa. In China’s totalitarian system the Elites directly implement their famous single child quota.
Sterilization ploys throughout history usually end up playing out as some sort of racists scheme. But the ultimate goal is self-administered population reduction methods such as abortion.
Method 9: Wars
Wars have the obvious effect of reducing human population, and what may not be so obvious is the benefit that comes to international bankers who fund both sides of wars through central banks.
Wars accomplish population reduction while at the same time enriching war profiteers. The world has always managed several fronts of wars at any given time. However, the war on terrorism promises perpetual wars with no end in sight and a rising death toll that comes with it.
Method 8: No cures for diseases
Today’s doctors are drug dealers for the large and powerful pharmaceutical companies. Human doctors might replaced by Artificially Intelligent machines.
Doctors remain powerless against Big Pharma, government regulatory bodies such as the FDA,
Any doctor who tries to be a real Doctor and actually cures people is discredited out of the profession.
Method 7: Sexually transmitted diseases
Sexually transmitted diseases (STD’s) such as HIV reduce human reproduction, shorten lifespan while creating a drug-dependent patient forced to buy treatments since cures are purposely withheld. The main goal of STD’s is to discourage pregnancies and create self-inflicted population control, which is a lot more efficient than forced population control.
Method 6: Environmental Manipulation
Pesticides and other chemical agents in the air that cause cancers, asthma, allergies and other sicknesses are very effective at making people sick and requiring them to buy medical treatments that make them even sicker.
Meanwhile, weather manipulation by DARPA and other agencies around the world directly result in disasters that appear natural and kill thousands of people at a time.
Method 5: Abortions
Abortions is the result of a perfectly executed population reduction campaign that resulted in self-execution. According to the World Health Organization, there are 40-50 million abortions per year worldwide, or about 125,000 abortions per day.
Method 4: Genetically Modified Organisms
Genetically Modified Organisms (GMO’s) such as insects, plants and animals is the future.
These GMO’s do all sorts of interesting new things such as mating with natural organisms to prevent them from producing natural seeds, using them as bioweapons and merging them with technology to carry out even more impressive missions against the human population.
Method 3: Same sex relationships
The explosion of same sex images in the media and Hollywood content is a planned and executed psychological operation (psyop).
This psyop conducted over the last 10 years on the human population has accomplished its mission of creating a self-executing population reduction paradigm.
Same sex relationships promise to be the most efficient human population reduction tool that ever existed.
Method 2: The food supply
If you control the food supply for any living organism, you control the organism, and humans are no different. The powerful have been slowly modifying the food of humans with all sorts of hormones, antibiotics and God knows what else for both profit and to affect physical change in the human body.
The most evident effect of food source manipulation is obesity, early menstruation in females, reduction of testosterone levels in men, and overall hormonal imbalance that causes sexual confusion and gender dyslexia. The combination of all this feeds right into the same sex relationship psychological operation against the human population to ultimately reduce the human reproduction rate.
Method 1: Transhumanism
— the merging of humans with sophisticated technologies that greatly enhance human intellectual, physical, and psychological capacities. Transhumanism would completely eliminate the need for human population control or reduction by other means, since the technological enhancements would allow the creators and administrators of the “transhumans” to literally control their body and mind.
SARS-CoV-2, the virus that causes COVID-19, is constantly changing and accumulating mutations in its genetic code over time. New variants of SARS-CoV-2 are expected to continue to emerge. Some variants will emerge and disappear, while others will emerge and continue to spread and may replace previous variants.
To identify and track SARS-CoV-2 variants, CDC uses genomic surveillance. CDC's national genomic surveillance system collects SARS-CoV-2 specimens for sequencing through the National SARS-CoV-2 Strain Surveillance (NS3) program, as well as SARS-CoV-2 sequences generated by commercial or academic laboratories contracted by CDC and state or local public health laboratories. Virus genetic sequences are analyzed and classified as a particular variant. The proportion of variants in a population are calculated nationally, by HHS region, and by jurisdiction. The thousands of sequences analyzed every week through CDC’s national genomic sequencing and bioinformatics efforts fuel the comprehensive and population-based U.S. surveillance system established to identify and monitor the spread of variants.
Rapid virus genomic sequencing data combined with phenotypic data are further used to determine whether COVID-19 tests, treatments, and vaccines authorized or approved for use in the United States will work against emerging variants.
(CNN)Unvaccinated people do more than merely risk their own health. They're also a risk to everyone if they become infected with coronavirus, infectious disease specialists say.
That's because the only source of new coronavirus variants is the body of an infected person.
"Unvaccinated people are potential variant factories," Dr. William Schaffner, a professor in the Division of Infectious Diseases at Vanderbilt University Medical Center, told CNN Friday.
"The more unvaccinated people there are, the more opportunities for the virus to multiply," Schaffner said.
edition.cnn.com [2021-07-06] By Maggie Fox, July 3, 2021 link archive General
There are now additional benefits to doing this too. We are introducing new technology in our labs to identify variants of COVID-19 so we can track the variants that emerge and spread in coming months. We can only do this with the samples taken for PCR.
publichealthmatters.blog.gov.uk [2021-07-06] Susan Hopkins,:30 March 2021 link archive General
With the emergence of SARS-CoV-2 variants that may confer an evolutionary advantage to the virus, the need for fast, sensitive, and reliable tests for researchers to monitor for variants is essential both for tracking purposes and sequencing prioritization.
The SARS-CoV-2 Variant Assays are predesigned mutation detection assays targeting the most prominent variants known to date. These are single-tube duplex assays designed to support detection of a specific mutation in the FAM channel and wild-type sequence in the HEX channel using either Droplet Digital PCR (ddPCR) or RT-PCR.
New assays are expected to be made available for research use as new variants emerge.
The current method for SARS-CoV-2 detection is based on RT-PCR. Briefly, this method uses a DNA probe that binds to the viral sequence, which is then amplified by DNA amplifying enzymes. The amplification is a signal for the presence of the virus.
DiaCarta’s SARS-CoV-2 detection method is also an RT-PCR-based method but instead of using a DNA probe, it uses an XNA probe. XNAs are synthetic nucleic acid analogs that are different from DNA only in their sugar backbone. They can hybridize with DNA and can be used in RT-PCR testing just like a DNA probe. XNAs, however, offer an advantage over conventional DNA probes in the detection of specific mutations.
Conventional RT-PCRs can also detect mutations, however, with low confidence. XNA technology, on the other hand, can detect them with high specificity. This is because the temperature at which XNA and DNA hybridize can drop dramatically if there is a change in DNA sequence such as in the case of a mutation.
This temperature change prevents amplification of DNA molecules without the mutation allowing highly specific amplification of just the mutated sequences. According to the publication, a single base-pair mismatch between XNA/DNA duplex can result in a drop of 10-18C in the melting temperature.
geneonline.news [2021-07-06] by Ruchi Jhonsa, 2021-04-23 link archive General
There are 4 current variants of concern (VOCs) and 10 variants under investigation (VUIs) (Table 1).
This report has been published to continue to share the detailed variant surveillance analyses which contribute to the variant risk assessments and designation of new VOCs and VUIs. The specialist technical briefings contain early data and analysis on emerging variants and findings have a high level of uncertainty.
[...]
assets.publishing.service.gov.uk [2021-08-10] (pdf doc) link archive General
Specimen receipt and initial processing: Specimens are received and entered into the laboratory information system.
Specimen preparation and sequencing: SARS-CoV-2 RNA is extracted and converted to complimentary DNA, enriched, and loaded into the next-generation sequencing equipment.
Sequence data generation and collection: Specimens are sequenced and data is collected from sequencers and initial quality control steps are taken. The raw data is processed and turned into sequence data. At this point, a parallel process begins where sequence data collected from commercial laboratories are integrated with CDC databases for processing.
Sequence data submission to public repositories: Scientists conduct quality control steps. Sequences not initially accepted by public repositories are analyzed and potentially re-sequenced for resubmission. Published data are made available to scientists around the world through public repositories.
CDC conducts genomic surveillance to track SARS-CoV-2 variants in the United States.
What is added by this report?
CDC’s SARS-CoV-2 genomic surveillance has been expanded to incorporate sequence data from public repositories and to produce weighted estimates of variant proportions at the jurisdiction level. The Delta (B.1.617.2 and AY sublineages) variant rose to predominance in late June 2021, followed by the rapid rise of Omicron (B.1.1.529 and BA sublineages) in December 2021.
What are the implications for public health practice?
The dynamic landscape of SARS-CoV-2 variants in 2021, including Delta- and Omicron-driven resurgences of SARS-CoV-2 transmission across the United States, underscores the importance of robust genomic surveillance efforts to inform public health planning and practice.
Genomic surveillance is a critical tool for tracking emerging variants of SARS-CoV-2 (the virus that causes COVID-19), which can exhibit characteristics that potentially affect public health and clinical interventions, including increased transmissibility, illness severity, and capacity for immune escape. During June 2021–January 2022, CDC expanded genomic surveillance data sources to incorporate sequence data from public repositories to produce weighted estimates of variant proportions at the jurisdiction level and refined analytic methods to enhance the timeliness and accuracy of national and regional variant proportion estimates. These changes also allowed for more comprehensive variant proportion estimation at the jurisdictional level (i.e., U.S. state, district, territory, and freely associated state). The data in this report are a summary of findings of recent proportions of circulating variants that are updated weekly on CDC’s COVID Data Tracker website to enable timely public health action.† The SARS-CoV-2 Delta (B.1.617.2 and AY sublineages) variant rose from 1% to >50% of viral lineages circulating nationally during 8 weeks, from May 1–June 26, 2021. Delta-associated infections remained predominant until being rapidly overtaken by infections associated with the Omicron (B.1.1.529 and BA sublineages) variant in December 2021, when Omicron increased from 1% to >50% of circulating viral lineages during a 2-week period. As of the week ending January 22, 2022, Omicron was estimated to account for 99.2% (95% CI = 99.0%–99.5%) of SARS-CoV-2 infections nationwide, and Delta for 0.7% (95% CI = 0.5%–1.0%). The dynamic landscape of SARS-CoV-2 variants in 2021, including Delta- and Omicron-driven resurgences of SARS-CoV-2 transmission across the United States, underscores the importance of robust genomic surveillance efforts to inform public health planning and practice.
In November 2020, CDC expanded its genomic surveillance program to track SARS-CoV-2 lineages at the national and U.S. Department of Health and Human Services (HHS) regional levels (1,2). CDC also initiated SARS-CoV-2 Sequencing for Public Health Emergency Response, Epidemiology, and Surveillance§ (SPHERES), a national SARS-CoV-2 genomic surveillance consortium. Currently, the national genomic surveillance program integrates three principal sources of SARS-CoV-2 sequence data: 1) the National SARS-CoV-2 Strain Surveillance (NS3) program¶; 2) CDC-contracted commercial sequencing data; and 3) sequences from public health, academic, and clinical laboratories that are tagged** as baseline surveillance in public genomic data repositories, such as Global Initiative on Sharing All Influenza Data (GISAID) and National Center for Biotechnology Information (NCBI) GenBank. Inclusion of tagged SARS-CoV-2 sequence data was instituted in October 2021 to enhance the geographic representativeness and precision of variant proportion estimates and to enhance the surveillance program’s sustainability.
SARS-CoV-2 consensus sequences†† submitted or tagged for national genomic surveillance were combined, assessed for quality, deduplicated, and analyzed for weekly estimation of variant proportions at the national, HHS regional, and jurisdictional levels. SARS-CoV-2 variant proportions (with 95% CIs) were estimated weekly for variants of concern, variants of interest, variants being monitored,§§ and any other lineages accounting for >1% of sequences nationwide during the preceding 12 weeks. Proportion estimation methods used a complex survey design with statistical weights to correct potential biases because samples selected for sequencing might not be representative of all SARS-CoV-2 infections (Box).¶¶ Each submitting laboratory source was considered a primary sampling unit, and the geographic level (i.e., jurisdictional, HHS regional, or national) and week of sample collection for each sequence, a stratum. Weights account for the probability that a sample from an infection is sequenced and are trimmed to the 99th percentile. Variant proportion estimates that did not meet the National Center for Health Statistics’ data presentation standards for proportions were flagged.*** During June 2021–January 2022, the median interval from SARS-CoV-2 sample collection to availability of consensus sequences was 15 days. Therefore, to estimate variant proportions during the most recent 2 weeks, multinomial regression models were fit for national and regional estimates to nowcast (2) variant proportions with corresponding 95% projection intervals††† using the most recent 21 weeks of data for prediction. To compare the speeds of initial variant transmission, the doubling time of each variant was calculated using the “time” covariate in nowcast models. All analyses used PANGO SARS-CoV-2 lineage nomenclature and sublineages were aggregated under the parent lineage (3). This activity was reviewed by CDC and conducted consistent with applicable federal law and CDC policy.§§§
[...]
cdc.gov [2022-10-19] Anastasia S. Lambrou, Philip Shirk, ..., David E. Wentworth, February 11, 2022 link archive General
New variants of the Covid-19(84) virus like “Delta” and “Lamda” (and an unlimited amount of others) are keeping a large part of society in a perpetual state of fear while news headlines claim if you’re one of the “unvaxed” you’re essentially doomed! But where are these variants coming from and is there actually a cause for concern? In this video Dan Dicks of Press For Truth reexamines his nearly 13 year old idea that the shot itself is the pandemic by analyzing current events and asking whether or not the same holds true in today’s Covid-19(84) nightmare!
Not all vaccines prevent infection. Some, known as leaky vaccines, prolong host survival or reduce disease symptoms without preventing viral replication and transmission. Although leaky vaccines provide anti-disease benefits to vaccinated individuals, new research by CIDD’s Andrew Read, David Kennedy and colleagues at the Avian Oncogenic Virus Group in the United Kingdom, and The University of New England in Australia, has demonstrated that leaky vaccines can make the situation for unvaccinated individuals worse. Leaky vaccines work by enhancing host immunity to a particular pathogen, without necessarily blocking or slowing viral replication. The result is that infected but vaccinated individuals have extended survival, allowing highly virulent pathogen that would normally reach an evolutionary dead-end in a dead host, can transmit. The evolutionary consequences of high virulence are thus reduced and these pathogens can be selectively favored as a result of leaky vaccination.
[...]
epidemics.psu.edu [2021-11-29] January 14, 2016 link archive General
Read and others, including researchers at the U.S. Department of Agriculture, posit that the virus that causes Marek’s has been changing over time in ways that helped it evade its previous vaccines. The big question is whether the vaccines directly incited these changes or the evolution happened, coincidentally, for other reasons, but Read is pretty sure the vaccines have played a role. In a 2015 paper in PLOS Biology, Read and his colleagues vaccinated 100 chickens, leaving 100 others unvaccinated. They then infected all the birds with strains of Marek’s that varied in how virulent — as in how dangerous and infectious — they were. The team found that, over the course of their lives, the unvaccinated birds shed far more of the least virulent strains into the environment, whereas the vaccinated birds shed far more of the most virulent strains. The findings suggest that the Marek’s vaccine encourages more dangerous viruses to proliferate. This increased virulence might then give the viruses the means to overcome birds’ vaccine-primed immune responses and sicken vaccinated flocks.
[...]
quantamagazine.org [2021-11-29] Melinda Wenner Moyer, May 10, 2018 link archive General
The importance of understanding SARS-CoV-2 evolution cannot be overlooked. Recent studies confirm that natural selection is the dominating mechanism of SARS-CoV-2 evolution, which favors mutations that strengthen viral infectivity. Here, we demonstrate that vaccine-breakthrough or antibody-resistant mutations provide a new mechanism of viral evolution. Specifically, vaccine-resistant mutation Y449S in the spike (S) protein receptor-binding domain, which occurred in co-mutations Y449S and N501Y, has reduced infectivity compared to that of the original SARS-CoV-2 but can disrupt existing antibodies that neutralize the virus. By tracking the evolutionary trajectories of vaccine-resistant mutations in more than 2.2 million SARS-CoV-2 genomes, we reveal that the occurrence and frequency of vaccine-resistant mutations correlate strongly with the vaccination rates in Europe and America. We anticipate that as a complementary transmission pathway, vaccine-breakthrough or antibody-resistant mutations, like those in Omicron, will become a dominating mechanism of SARS-CoV-2 evolution when most of the world's population is either vaccinated or infected. Our study sheds light on SARS-CoV-2 evolution and transmission and enables the design of the next-generation mutation-proof vaccines and antibody drugs.
[...]
pubmed.ncbi.nlm.nih.gov [2021-12-08] Rui Wang, Jiahui Chen, Guo-Wei Wei, Dec 7, 2021 link archive General
The CDC continues to claim that it is a “myth” that “COVID-19 vaccines cause variants.” ICAN filed a Freedom of Information Act request asking for its evidence that vaccines do not cause variants. You won’t believe what they said.
This letter is in response to your Centers for Disease Control and Prevention and Agency for Toxic Substances and Disease Registry (CDC/ATSDR) Freedom of Information Act (FOIA) request of March 8, 2022, for “all documents sufficient to support that the immunity conferred by COVID-19 vaccines does not contribute to virus evolution and the emergence of variants.”
A search of our records failed to reveal any documents pertaining to your request. The CDC’s Emergency Operations Center and the National Center for Immunization and Respiratory Diseases conducted searches and found no records responsive to your request.
[...]
thehighwire.com [2022-05-19] The HIGHWIRE, May 13, 2022 link archive General
See related data element: Imperfect Vaccination Can Enhance the Transmission of Highly Virulent Pathogens
The vaccinal antibodies are not matching the circulating virus and sub-variants/clades and this causes viral immune escape, selecting for variants that could overcome the sub-optimal immune response
It is as if the vaccine, this COVID vaccine, gene injection, and the roll-out, was designed to fail. Day one!
Moreover, the same capacity for the induced ‘antigen-specific’ high affinity vaccinal antibodies to overcome the sub-optimal immune pressure and select for variants that are more ‘infectious’ e.g. omicron, is the same process that will work on overcoming blocking of virus virulence in the distal lower lung. And as such, select for sub-variants that could cause severe ‘virulent’ lethal disease in the lower respiratory tract. We may be on the tip of very serious disease (I speak to GVB routinely) from COVID based on continuation of this mass vaccination with these sub-optimal vaccines.
It is as if the vaccine people, the government alphabet agencies, Fauci, Walensky, Francis Collins etc., the CDC, NIH, Pfizer do not know what they are doing. And it is basic.
Darwinian Natural Selection will cause the selection of variants that are more and more infectious and ‘fitter’ and one can emerge that is even more virulent and lethal.
We usually do not vaccinate across a full population for all age-groups. We focus to the high-risk vulnerable elderly population as an example. Or only children.
[...]
palexander.substack.com [2022-11-06] Dr. Paul Alexander, November 5, 2022 link archive General
Investigative Journalist with a popular Substack, Igor Chudov, explains his recent discoveries comparing the dramatic difference in Covid-19 death rates in both Portugal and South Africa, and what could be the cause.
Associations between vaccine breakthrough cases and infection by different SARS coronavirus 2 (SARS-CoV-2) variants have remained largely unexplored. Here we analysed SARS-CoV-2 whole-genome sequences and viral loads from 1,373 persons with COVID-19 from the San Francisco Bay Area from 1 February to 30 June 2021, of which 125 (9.1%) were vaccine breakthrough infections. Vaccine breakthrough infections were more commonly associated with circulating antibody-resistant variants carrying ≥1 mutation associated with decreased antibody neutralization (L452R/Q, E484K/Q and/or F490S) than infections in unvaccinated individuals (78% versus 48%, P = 1.96 × 10−8). Differences in viral loads were non-significant between unvaccinated and fully vaccinated cases overall (P = 0.99) and according to lineage (P = 0.09–0.78). Symptomatic vaccine breakthrough infections had comparable viral loads (P = 0.64), whereas asymptomatic breakthrough infections had decreased viral loads (P = 0.023) compared with infections in unvaccinated individuals. In 5 cases with serial samples available for serologic analyses, vaccine breakthrough infections were found to be associated with low or undetectable neutralizing antibody levels attributable to an immunocompromised state or infection by an antibody-resistant lineage. Taken together, our results show that vaccine breakthrough infections are overrepresented by antibody-resistant SARS-CoV-2 variants, and that symptomatic breakthrough infections may be as efficient in spreading COVID-19 as unvaccinated infections, regardless of the infecting lineage.
[...]
nature.com [2022-07-27] Venice Servellita, Mary Kate Morris, ..., Charles Y. Chiu, January 10, 2022 link archive General
How can I tell if I have the Delta variant? Do labs report that to the state?
That information may not be readily available. The viral tests that are used to determine if a person has COVID-19 are not designed to tell you what variant is causing the infection. Detecting the Delta variant, or other variants, requires a special type of testing called genomic sequencing. Due to the volume of COVID-19 cases, sequencing is not performed on all viral samples. However, because the Delta variant now accounts for the majority of COVID-19 cases in the United States, there is a strong likelihood that a positive test result indicates infection with the Delta variant.
[...]
dshs.state.tx.us [2021-09-01] Last updated: August 11, 2021 link archive General
Washington — As the U.S. continues to navigate its way through the COVID-19 pandemic, Dr. Scott Gottlieb, the former commissioner of the Food and Drug Administration, said areas of the country could experience "very dense outbreaks" with the concerning Delta variant continuing to circulate.
msn.com [2021-06-29] Kimani Hayes, June 28, 2021 link archive General
An investigation is underway into how a care home in Nivelles in Walloon Brabant came to be infected with the Delta variant of the coronavirus, while 95% of the residents and 75% of staff were fully vaccinated.
brusselstimes.com [2021-07-06] By Alan Hope, 24 June 2021 link archive General
All told, Israeli government data show the Pfizer vaccine is indeed significantly less effective at preventing coronavirus cases of the delta variant (64 percent) than it was for previous variants (95 percent). It’s also significantly less effective at preventing symptomatic cases (64 percent vs. 97 percent). But it performs much more similarly when it comes to preventing serious cases and hospitalization (93 percent vs. 97.5 percent).
In other words, the delta variant means the virus will probably continue to spread, even among vaccinated people and even in a strongly vaccinated country such as Israel, because the vaccines don’t protect from transmission or symptomatic cases nearly as well. But that doesn’t mean the vaccines don’t work, especially when it comes to preventing the worst of the disease.
[...]
washingtonpost.com [2021-07-22] By Aaron Blake, July 19, 2021 link archive General
What has emerged from 19 months of work, backed by decades of coronavirus research, is a blow-by-blow account of how SARS-CoV-2 invades human cells (see ‘Life cycle of the pandemic coronavirus’). Scientists have discovered key adaptations that help the virus to grab on to human cells with surprising strength and then hide itself once inside. Later, as it leaves cells, SARS-CoV-2 executes a crucial processing step to prepare its particles for infecting even more human cells. These are some of the tools that have enabled the virus to spread so quickly and claim millions of lives. “That’s why it’s so difficult to control,” says Wendy Barclay, a virologist at Imperial College London.
[...]
nature.com [2021-08-04] Megan Scudellari, 28 July 2021 link archive General
"Some vaccinated people infected with the Delta variant after vaccination may be contagious and spread the virus to others," Walensky said, during a CDC press call Tuesday afternoon, saying that "new scientific data" on Delta has prompted the change.
[...]
businessinsider.com [2021-08-05] Hilary Brueck, Jul 28, 2021 link archive General
(NEXSTAR) – So you’ve tested positive for COVID – but which COVID exactly? Is there a way to tell if you have the highly transmissible delta variant?
There is a way to tell, but there’s not really a way for you to tell. Test results from a PCR or antigen test you might take at a testing site or in a take-home kit will only tell you if you’re positive or negative for the new coronavirus that causes COVID-19.
[...]
fox46.com [2021-08-14] Alix Martichoux, Aug 8, 2021 link archive General
The rise of the Delta variant of the coronavirus has raised new questions about how the vaccinated can stay safe and avoid breakthrough infections. We asked the experts for advice.
nytimes.com [2021-08-14] By Tara Parker-Pope, Aug 3, 2021 link archive General
mRNA-based vaccines provide effective protection against most common SARS-CoV-2 variants. However, identifying likely breakthrough variants is critical for future vaccine development. Here, we found that the Delta variant completely escaped from anti-N-terminal domain (NTD) neutralizing antibodies, while increasing responsiveness to anti-NTD infectivity-enhancing antibodies. Although Pfizer-BioNTech BNT162b2-immune sera neutralized the Delta variant, when four common mutations were introduced into the receptor binding domain (RBD) of the Delta variant (Delta 4+), some BNT162b2-immune sera lost neutralizing activity and enhanced the infectivity. Unique mutations in the Delta NTD were involved in the enhanced infectivity by the BNT162b2-immune sera. Sera of mice immunized by Delta spike, but not wild-type spike, consistently neutralized the Delta 4+ variant without enhancing infectivity. Given the fact that a Delta variant with three similar RBD mutations has already emerged according to the GISAID database, it is necessary to develop vaccines that protect against such complete breakthrough variants.
An outbreak of severe acute respiratory syndrome coronavirus 2 caused by the Gamma variant of concern infected 24/44 (55%) employees of a gold mine in French Guiana (87% symptomatic, no severe forms). The attack rate was 60% (15/25) among fully vaccinated miners and 75% (3/4) among unvaccinated miners without a history of infection.
[...]
In conclusion, we describe a VOC Gamma COVID-19 outbreak with a strikingly high attack rate among persons fully vaccinated with BNT162b2 vaccine. Our observation suggested that BNT162b2 protected from severe COVID-19. However, this single unexpected outbreak in a small and isolated vaccinated population requires further real-life studies on BNT162b2 vaccine effectiveness against the VOC Gamma. Masking and social distancing —even among those fully vaccinated— may be necessary among persons with frequent exposure in Gamma variant–endemic zones.
[...]
wwwnc.cdc.gov [2021-09-02] Nicolas Vignier, ..., Loïc Epelboin, Page created: July 15, 2021, Page updated: July 21, 2021 link archive General
As the US struggles to suppress the rapidly advancing coronavirus Delta variant, new evidence has emerged that the latest Lambda mutation — ravaging parts of South America — won’t be slowed by vaccines.
In a July 28 report appearing on bioRxiv, where the study awaits peer review prior to getting published, researchers in Japan are sounding the alarm on the C.37 variant, dubbed Lambda. And it’s proven just as virulent as Delta thanks to a similar mutation making them even more contagious.
The strain has been contained in 26 countries, including substantial outbreaks in Chile, Peru, Argentina and Ecuador.
“Notably, the vaccination rate in Chile is relatively high; the percentage of the people who received at least one dose of COVID-19 vaccine was [about] 60%,” the authors write.
[...]
nypost.com [2021-08-14] By Hannah Sparks, August 12, 2021 link archive General
CDC has been collaborating with global public health and industry partners to learn about Omicron, as we continue to monitor its course. We don’t yet know how easily it spreads, the severity of illness it causes, or how well available vaccines and medications work against it.
Spread
The Omicron variant likely will spread more easily than the original SARS-CoV-2 virus and how easily Omicron spreads compared to Delta remains unknown. CDC expects that anyone with Omicron infection can spread the virus to others, even if they are vaccinated or don’t have symptoms.
Severe Illness
More data are needed to know if Omicron infections, and especially reinfections and breakthrough infections in people who are fully vaccinated, cause more severe illness or death than infection with other variants.
Vaccines
Current vaccines are expected to protect against severe illness, hospitalizations, and deaths due to infection with the Omicron variant. However, breakthrough infections in people who are fully vaccinated are likely to occur. With other variants, like Delta, vaccines have remained effective at preventing severe illness, hospitalizations, and death. The recent emergence of Omicron further emphasizes the importance of vaccination and boosters.
[...]
cdc.gov [2022-01-11] As of: Dec. 20, 2021 link archive General
Scientists have raised concerns about a new variant of coronavirus that has an "extremely high number" of mutations that vaccines may not protect the human body against.
The B.1.1.529 variant was first detected in Botswana, Africa in November with subsequent infections confirmed through genome sequencing in South Africa and in a traveller from Hong Kong after returning from the Rainbow Nation.
Only ten cases have been reported across the world but health experts believe it could have spread further than three countries as nations ease COVID-19 restrictions and restart international travel.
[...]
skynews.com.au [2021-11-29] David Wu, November 25, 2021 link archive General
As more data revels less benefit to vaccination status; and additional data reveals vaccinated individuals are becoming the group with the most adverse health outcomes; the scientific and medical community -writ large- are facing increased scrutiny to justify the public benefit of a seemingly endless booster approach with little upside.
In essence, what good are all these vaccinations; and specifically all the rules of proving your vaccinated status vis-a-vis passports; if the vaccinated can still be infected and spread the virus? The voices asking this question are growing more loud by the day. Then, all of a sudden….
theconservativetreehouse.com [2021-11-29] November 24, 2021 link archive General
What a small world we live in. The “Nu variant” scare you keep hearing about is coming from the same people and institutions that spawned the last COVID scare, and the one before that, and the one before that one, dating back all the way to the onset of COVID Mania.
[Update: the World Health Organization has now labeled this strain the “Omicron variant,” in noticeably skipping over “Xi” in the greek alphabet]
[...]
dossier.substack.com [2021-11-29] Jordan Schachtel, Nov 27, 2021 link archive General
Travellers arriving in England from several southern African countries will have to quarantine amid warnings over a new coronavirus variant.
UK Health Secretary Sajid Javid said from 12:00 GMT on Friday six countries would be added to the red list, with flights being temporarily banned.
One expert described the variant, known as B.1.1.529, as "the worst one we've seen so far", and there is concern it has the potential to evade immunity.
No cases have been confirmed in the UK.
Only 59 confirmed cases have been identified in South Africa, Hong Kong and Botswana so far.
Update (1008ET):Reuters reports BioNTech, Pfizer is expecting laboratory results of the recently discovered Nu variant in two weeks.
"We understand the concern of experts and have immediately initiated investigations on variant B.1.1.529," BioNTech said.
"We expect more data from the laboratory tests in two weeks at the latest. These data will provide more information about whether B.1.1.529 could be an escape variant that may require an adjustment of our vaccine if the variant spreads globally," it added.
[...]
zerohedge.com [2021-11-29] NOV 26, 2021 link archive General
Countering global alarmism about the omicron variant of COVID-19, the doctor who first discovered it says the strain is “mild” and hasn’t caused an uptick in hospitalizations.
Governments across the world are imposing new travel bans and other virus restrictions in response to claims the new strain is more transmissible and could prove more deadly than delta.
However, those with the most expertise on the ground in South Africa are all saying the opposite.
Barry Schoub, chairman of the Ministerial Advisory Committee on Vaccines, told Sky News that the panic had been misplaced.
As public health officials stir up fear about the latest new COVID variant, experts warn vaccines are maiming and killing young people in alarming numbers.
Just in time for the end-of-year holidays, Centers for Disease Control and Prevention (CDC) officials and their bought media agents trotted out a new round of Gothic horror stories about a purported COVID “variant.”
Their apparent hope is that the synchronized hullabaloo about “variants” will distract the public from the true nightmare that is unfolding: a record-setting uptick in all-cause mortality that jives suspiciously not only with the timing of the COVID vaccination rollout but with the top adverse events — heart failure, heart disease, circulatory conditions and strokes — associated with the experimental COVID shots.
Media reports acknowledge the rising tide of “extra non-COVID deaths” and “seriously ill people” swarming emergency departments, even stating that patients are “showing up much sicker than [ER staff have] ever seen” and are younger than expected.
However, while admitting patients’ unusual symptoms — abdominal pain, blood clots, heart conditions and tingling of extremities — are not COVID-related, health officials assert “no one knows why” they are occurring.
For others, the explanation is obvious. “These are precisely the ailments one would expect to see,” said Mike Whitney of The Unz Review, “if one had just injected millions of people with a clot-generating biologic that triggers a violent immune response that attacks the inner lining of the blood vessels inflicting severe damage to the body’s critical infrastructure.”
UCLA pediatric specialist J. Patrick Whelan, M.D., Ph.D., gave the U.S. Food and Drug Administration (FDA) ample warning about this very scenario back in December 2020.
At the time, Whelan was already deeply concerned about the risk of “long-lasting or even permanent damage to [the] brain or heart microvasculature” from clotting and inflammation induced by the spike protein-based vaccines.
By July 2021, Canadian physician Dr. Charles Hoffe was in complete agreement. Hoffe’s experience with COVID-vaccinated patients indicated that not only is “widespread microscopic blood clotting” a virtually “inevitable” outcome of the mRNA vaccines, but “the worst,” in all likelihood, “is yet to come.”
South African physician Dr. Shankara Chetty recently termed the vaccines’ synthetic spike protein “one of the most contrived poisons that man has ever made.”
[...]
childrenshealthdefense.org [2021-12-12] 12/01/21 link archive General
On Sky News Breakfast with Kay Burley on Thursday December 16: [... at 5:42, Gillian Keegan is interviewed and reveals astonishing low numbers triggering alarm.]
Public officials and media reported that a man in Texas became the first American to die from the Omicron variant. I checked with the Harris County Public Health Department. Turns out that's not true.
Health chief accused of disseminating misleading statistics on hospitalisations that overstated the risk from omicron
One of Britain’s most senior health advisers has been accused of disseminating “dodgy data” that inflated the potential risk of omicron.
Dr Jenny Harries, the chief executive of the UK Health Security Agency (UKHSA), is understood to have been the source of a contested claim by Sajid Javid, the Health Secretary, that there is typically a 17-day lag between patients becoming infected and requiring hospitalisation.
However, independent experts pointed to Office for National Statistics (ONS) data, which suggested an average delay of nine or 10 days.
The claim by Mr Javid was seen as an attempt to strengthen the case for urgent new Covid-19 restrictions, on the basis that the country could be on the brink of a major spike in hospitalisations due to omicron.
Dr Harries has claimed that omicron was “probably the most significant threat we’ve had since the start of the pandemic”.
Health and scientific advisers have been pushing for lockdown measures and Boris Johnson will have to urgently decide whether or not to impose new restrictions before the New Year.
[...]
telegraph.co.uk [2021-12-26] By Edward Malnick, December 25, 2021 link archive General
For a while now it’s been clear the primary objective of most pandemic coverage is to scare the socks off mass audiences. Good news, bad news, boring news, interesting news, news that’s more of a wash in the final analysis, news that’s a net plus overall: it’s all presented as terrifying, more signs of the Apocalypse. There’s no better example than the stampede to advertise the “first death from Omicron” in the United States.
Matt Orfalea does a hilarious job of stitching together an homage to the latest moral panic. So many great little details here, from the “Way Too Early” background to one reporter’s premature death report to the “aggressive Covid vice” imagery, the dramatic Biden-cough, and so much more.
Omicron largely evades immunity from past infection or two vaccine doses, according to Imperial's latest report.
The new report from the Imperial College London COVID-19 response team estimates that the risk of reinfection with the omicron variant is 5.4 times greater than that of the delta variant. This implies that the protection against reinfection by omicron afforded by past infection may be as low as 19%.
Researchers estimate the growth and immune escape of the omicron variant in England. They used data from the UKHSA and NHS for all PCR-confirmed SARS-CoV-2 cases in England who had taken a COVID test between November 29th and December 11th 2021.
he study includes people identified as having omicron infection due to an S gene target failure (SGTF), as well as people with genotype data that confirmed omicron infection. Overall, 196,463 people without S gene target failure (likely to be infected with another variant) and 11,329 cases with it (likely to be infected with omicron) were included in the SGTF analysis, as well as 122,063 delta and 1,846 omicron cases in the genotype analysis.
Dec. 22, 2021 -- People who get COVID-19 infections caused by the Omicron variant are less likely to need hospital care, compared with those infected by the Delta variant, according to two large new studies from the U.K. and South Africa.
The findings, which were released ahead of peer review, add to previous glimmers of evidence suggesting that Omicron -- while extremely contagious -- may result in less severe symptoms than its predecessors.
“This is helping us quantify how much less severe Omicron is than Delta, and it appears to be between 40 to 75% reduced risk of hospitalizations, adjusted for many factors, which is very good,” said Eric Topol, MD, the editor-in-chief of Medscape and a cardiologist at Scripps Research Translational Institute in La Jolla, CA.
The first analysis, which was done by the World Health Organization Collaborating Centre for Infectious Disease Modelling and Imperial College London, found that overall, people infected by Omicron had about a 20% reduced risk of needing any hospital care for their infections and a 40% lower risk of an overnight hospital stay, compared to those infected with Delta.
Meanwhile, people who were re-infected -- meaning they caught Omicron after recovering from a previous COVID-19 infection -- had a 50%-60% lower risk of needing hospital care, likely reflecting the benefits of having some prior immunity against the same family of viruses.
The study included everyone with polymerase chain reaction-confirmed COVID-19 in the U.K. during the first 2 weeks of December -- roughly 56,000 Omicron cases and 269,000 Delta infections.
The second study, from researchers at the National Institute for Communicable Diseases in South Africa, included more than 29,000 COVID-19 cases that had lab results highly suggestive of Omicron infections. Compared to people infected with the Delta variant, those with presumed Omicron infections were about 70% less likely to have severe disease.
While the news is hopeful for individuals, on a population level, health care systems may still be stressed, the study authors warned.
[...]
webmd.com [2022-01-07] By Brenda Goodman, Dec. 22, 2021 link archive General
As many as 20% of all child deaths from Covid in the US have occurred during the Omicron surge of the pandemic.
Children seem to be facing increasing risks from Covid-19 even as mask mandates drop across the country, and vaccination rates among children stall out at alarmingly low rates.
“We saw a massive surge of hospitalized young children during Omicron that we didn’t see in the earlier months of the pandemic,” said Jason Kane, a pediatric intensivist and associate professor of pediatrics at the University of Chicago Comer children’s hospital.
Omicron was first identified in November, and within weeks became the dominant variant in the US.
Since the beginning of the current year, 179 children have died from Covid-19 in the US, compared with 735 children in the preceding 20 months, according to data from the American Academy of Pediatrics (AAP). The figures mainly involve the age group 0-17 and were gathered from about May of 2020 to early March 2022.
Scientists say Omicron appears to have a clear lab origin
Future lab releases of Covid-19 variants are “likely”
When Omicron emerged, many scientists were bowled over by the lightning speed with which it spread. Although public health officials had warned that the original Covid-19 was highly contagious and fast-moving— it looked like it was standing still next to the Omicron variant.
Now, some scientists examining the virus have concluded “vast” genetic mutations that likely occurred in a lab setting are what makes Omicron spread so quickly.
Omicron was first detected in Botswana, South Africa, reported to have been brought by a foreign delegation from a country officials will not identify, making it more difficult for outside observers to track its origin.
To many scientists, the genetic differences that made Omicron so quickly transmissible caused it to immediately stand out as unlikely to be a result of a natural evolution. Some note the “rapid accumulation of mutations in the SARS-CoV-2 Omicron variant that enabled its outbreak.”
[...]
sharylattkisson.com [2022-03-31] BY SHARYL ATTKISSON, MARCH 26, 2022 link archive General
NEW YORK, June 17 (Reuters) - People infected with the earliest version of the Omicron variant of the coronavirus, first identified in South Africa in November, may be vulnerable to reinfection with later versions of Omicron even if they have been vaccinated and boosted, new findings suggest.
Vaccinated patients with Omicron BA.1 breakthrough infections developed antibodies that could neutralize that virus plus the original SARS-CoV-2 virus, but the Omicron sublineages circulating now have mutations that allow them to evade those antibodies, researchers from China reported on Friday in Nature.
Several sublineages of omicron have emerged with additional mutations that may afford further antibody evasion. Here, we characterise the sensitivity of emerging omicron sublineages BA.2.75.2, BA.4.6, and BA.2.10.4 to antibody-mediated neutralisation, and identify extensive escape by BA.2.75.2. BA.2.75.2 was resistant to neutralisation by Evusheld (tixagevimab + cilgavimab), but remained sensitive to bebtelovimab. In recent serum samples from blood donors in Stockholm, Sweden, BA.2.75.2 was neutralised, on average, at titers approximately 6.5-times lower than BA.5, making BA.2.75.2 the most neutralisation resistant variant evaluated to date. These data raise concerns that BA.2.75.2 may effectively evade humoral immunity in the population.
biorxiv.org [2022-10-07] Daniel J. Sheward, Changil Kim, Julian Fischbach, Sandra Muschiol, Roy A. Ehling, Niklas K. Björkström, Gunilla B. Karlsson Hedestam, Sai T. Reddy, Jan Albert, Thomas P. Peacock, Ben Murrell, September 19, 2022 link archive General
The Omicron variants boast the highest infectivity rates among all SARS-CoV-2 variants. Despite their lower disease severity, they can reinfect COVID-19 patients and infect vaccinated individuals as well. The high number of mutations in these variants render them resistant to antibodies that otherwise neutralize the spike protein of the original SARS-CoV-2 spike protein. Recent research has shown that despite its strong immune evasion, Omicron still induces strong T Cell responses similar to the original variant. This work investigates the molecular basis for this observation using the neural network tools NetMHCpan-4.1 and NetMHCiipan-4.0. The antigens presented through the MHC Class I and Class II pathways from all the notable SARS-CoV-2 variants were compared across numerous high frequency HLAs. All variants were observed to have equivalent T cell antigenicity. A novel positive control system was engineered in the form of spike variants that did evade T Cell responses, unlike Omicron. These evasive spike proteins were used to statistically confirm that the Omicron variants did not exhibit lower antigenicity in the MHC pathways. These results suggest that T Cell immunity mounts a strong defense against COVID-19 which is difficult for SARS-CoV-2 to overcome through mere evolution.
biorxiv.org [2022-12-22] Arnav Solanki, James Cornette, Julia Udell, George Vasmatzis, Marc Riedel, November 10, 2022 link archive General
Importance: While a substantial fraction of the US population was infected with SARS-CoV-2 during December 2021 - February 2022, the subsequent evolution of population immunity against SARS-CoV-2 Omicron variants reflects the competing influences of waning protection over time and acquisition or restoration of immunity through additional infections and vaccinations.
Objective: To estimate changes in population immunity against infection and severe disease due to circulating SARS-CoV-2 Omicron variants in the United States from December 2021 to November 2022, and to quantify the protection against a potential 2022-2023 winter SARS-CoV-2 wave.
Design setting participants: Bayesian evidence synthesis of reported COVID-19 data (diagnoses, hospitalizations), vaccinations, and waning patterns for vaccine- and infection-acquired immunity, using a mathematical model of COVID-19 natural history.
Main outcomes and measures: Population immunity against infection and severe disease from SARS-CoV-2 Omicron variants in the United States, by location (national, state, county) and week.
Results: By November 9, 2022, 94% (95% CrI, 79%-99%) of the US population were estimated to have been infected by SARS-CoV-2 at least once. Combined with vaccination, 97% (95%-99%) were estimated to have some prior immunological exposure to SARS-CoV-2. Between December 1, 2021 and November 9, 2022, protection against a new Omicron infection rose from 22% (21%-23%) to 63% (51%-75%) nationally, and protection against an Omicron infection leading to severe disease increased from 61% (59%-64%) to 89% (83%-92%). Increasing first booster uptake to 55% in all states (current US coverage: 34%) and second booster uptake to 22% (current US coverage: 11%) would increase protection against infection by 4.5 percentage points (2.4-7.2) and protection against severe disease by 1.1 percentage points (1.0-1.5).
Conclusions and relevance: Effective protection against SARS-CoV-2 infection and severe disease in November 2022 was substantially higher than in December 2021. Despite this high level of protection, a more transmissible or immune evading (sub)variant, changes in behavior, or ongoing waning of immunity could lead to a new SARS-CoV-2 wave.
Key points: Question: How did population immunity against SARS-CoV-2 infection and subsequent severe disease change between December 2021, and November 2022?Findings: On November 9, 2022, the protection against a SARS-CoV-2 infection with the Omicron variant was estimated to be 63% (51%-75%) in the US, and the protection against severe disease was 89% (83%-92%).Meaning: As most of the newly acquired immunity has been accumulated in the December 2021-February 2022 Omicron wave, risk of reinfection and subsequent severe disease remains present at the beginning of the 2022-2023 winter, despite high levels of protection.
pubmed.ncbi.nlm.nih.gov [2023-02-06] Fayette Klaassen, Melanie H Chitwood, Ted Cohen, Virginia E Pitzer, Marcus Russi, Nicole A Swartwood, Joshua A Salomon, Nicolas A Menzies, November 2022 link archive General
Europe faces prospect of further Covid measures later in the year as share of Omicron BA.5 cases rise in Portugal and Germany
A spike of Covid-19 cases and deaths in Portugal driven by the Omicron BA.5 subvariant in spite of warm temperatures is causing capitals across Europe to once again consider measures against a pandemic that has started to fade into public memory.
Portugal confirmed 26,848 new cases and recorded 47 Covid deaths on Wednesday – the highest daily death toll since 17 February, when 51 deaths from the disease were reported.
The trend contrasts with the pandemic situation in France, Germany, the UK and neighbouring Spain, where case rates have been declining for the last two months.
[...]
theguardian.com [2022-06-29] Philip Oltermann, June 3, 2022 link archive General
‘It’s an unpredictable and unstable situation,’ says immune system expert Prof. Cyrille Cohen, urging lawmakers to ‘actively encourage herd immunity among the vulnerable’
The number of coronavirus patients in serious condition in Israel reached 140 on Friday, marking a near 70% rise since last week, with health experts warning that the current situation was “unstable.”
While Israel has seen rising infection numbers for a few weeks, a rise in seriously ill patients marks a real concern as the country deals with the spread of the new variant BA.5, with experts warning that hospitals may need to reopen COVID wards. The number was up from 85 seriously ill patients on Friday last week.
Some 7,313 Israelis tested positive for the virus on Friday, the Health Ministry said. The reproduction number (R) stood at 1.31 as of Friday. The figure measures how many people each coronavirus carrier infects on average, with any number above 1 meaning the spread of COVID-19 is increasing. It first began to rise above 1 in mid-May, having stayed below that threshold for nearly two months.
[...]
timesofisrael.com [2022-06-29] 17 June 2022 link archive General
Scientists fear the sub-variants may be similar to the more deadly Alpha and Delta variants
The latest sub-variants of Omicron may have evolved to target the lung, prompting fears the next wave of the Covid could be starting.
Hospital admissions for Covid patients in England have begun to grow again, new NHS data shows.
The World Health Organisation has been investigating two Omicron sub-variants since April to assess whether they are more infectious or dangerous than their predecessor. Both BA.4 and BA.5 have been added to the agency’s monitoring list.
[...]
independent.co.uk [2022-06-29] Thomas Kingsley, June 24, 2022 link archive General
After the global spread of SARS-CoV-2 Omicron BA.2 lineage, some BA.2-related variants that acquire mutations in the L452 residue of spike protein, such as BA.2.9.1 and BA.2.13 (L452M), BA.2.12.1 (L452Q), and BA.2.11, BA.4 and BA.5 (L452R), emerged in multiple countries. Our statistical analysis showed that the effective reproduction numbers of these L452R/M/Q-bearing BA.2-related Omicron variants are greater than that of the original BA.2. Neutralization experiments revealed that the immunity induced by BA.1 and BA.2 infections is less effective against BA.4/5. Cell culture experiments showed that BA.2.12.1 and BA.4/5 replicate more efficiently in human alveolar epithelial cells than BA.2, and particularly, BA.4/5 is more fusogenic than BA.2. Furthermore, infection experiments using hamsters indicated that BA.4/5 is more pathogenic than BA.2. Altogether, our multiscale investigations suggest that the risk of L452R/M/Q-bearing BA.2-related Omicron variants, particularly BA.4 and BA.5, to global health is potentially greater than that of original BA.2.
[...]
biorxiv.org [2022-06-29] Izumi Kimura, Daichi Yamasoba, Tomokazu Tamura, ..., May 26, 2022 link archive General
COVID-19 positivity rates are back above 20% in parts of Manhattan, as the latest city data indicate the virus is digging in ahead of winter.
The rolling seven-day positivity rate in the Hell's Kitchen area of Manhattan is up to 22.5%, according to city data Wednesday. That is by far the highest rate in New York City, and no other neighborhood is close. Just a day prior, no neighborhood was over 20%.
At the same time, the transmission rate in Manhattan, at 172.7 new cases per every 100,000 people over the last seven days, is up 7% in the last two weeks. As of Wednesday, the borough with the highest overall positivity percentage is Staten Island, with a seven-day average of 6.89%.
Citywide, the seven-day average of new daily confirmed and probable cases fell steadily all summer until early September, but since then has been stuck in a steady range between about 1,800 and 2,200 new cases a day.
Over the last few days, it has held very steady around 2,000 cases daily.
COVID Variants of Concern
Two new COVID-19 variants that quietly emerged on the scene over the last few weeks -- ones that Dr. Anthony Fauci has described as "pretty troublesome" -- are becoming increasingly prevalent in the New York area and stoking fresh concerns as the nation braces for yet another potential winter surge, the latest CDC data shows.
You may not have heard of these two subvariants before -- BQ.1 and BQ.1.1. Both are descendants of omicron, which has proven to be the most vaccine-elusive and infectious COVID variant to date, and both are spreading at rapid rates.
That's especially true in the CDC's New York region, which also includes New Jersey, Puerto Rico and the Virgin Islands. According to the health agency's latest variant report, those subvariants account for 11.6% and 8% (19.6%), respectively, of COVID cases for the week ending Oct. 15, up from 4.1% and 1.9% (6%) in the report two weeks prior.
The CDC estimates those two variants could account for up to 36.6% of New York area cases, which is nearly double the highest-range estimate at the national level.
nbcnewyork.com [2022-10-20] October 19, 2022 link archive General
Continuous evolution of Omicron has led to numerous subvariants that exhibit growth advantage over BA.5. Such rapid and simultaneous emergence of variants with enormous advantages is unprecedented. Despite their rapidly divergent evolutionary courses, mutations on their receptor-binding domain (RBD) converge on several hotspots, including R346, K356, K444, L452, N460K and F486. The driving force and destination of such convergent evolution and its impact on humoral immunity established by vaccination and infection remain unclear. Here, we demonstrate that these convergent mutations can cause striking evasion of convalescent plasma, including those from BA.5 breakthrough infection, and existing antibody drugs, including Evusheld and Bebtelovimab. BR.2, CA.1, BQ.1.1, BM.1.1.1, and especially XBB, are the most antibody-evasive strain tested, far exceeding BA.5 and approaching SARS-CoV-1 level. To delineate the origin of the convergent evolution, we determined the escape mutation profiles and neutralization activity of monoclonal antibodies (mAbs) isolated from BA.2 and BA.5 breakthrough-infection convalescents. Importantly, due to humoral immune imprinting, BA.2 and especially BA.5 breakthrough infection caused significant reductions in the epitope diversity of neutralizing antibodies and increased proportion of non-neutralizing mAbs, which in turn concentrated humoral immune pressure and promoted the convergent RBD evolution. Additionally, the precise convergent RBD mutations and evolution trends of BA.2.75/BA.5 subvariants could be inferred by integrating the neutralization-weighted DMS profiles of mAbs from various immune histories (3051 mAbs in total). Moreover, we demonstrated that as few as five additional convergent mutations based on BA.5 or BA.2.75 could completely evade most plasma samples, including those from BA.5 breakthrough infection, while retaining sufficient hACE2-binding affinity. These results suggest that current herd immunity and BA.5 vaccine boosters may not provide sufficiently broad protection against infection. Broad-spectrum SARS-CoV-2 vaccines and NAb drugs development should be of high priority, and the constructed convergent mutants could serve to examine their effectiveness in advance.
We have said months now the bivalent booster WILL fail and will not work well: original antigenic sin (hidden antigenic sin), antibody-dependent enhancement of infection & disease, viral immune escape
biorxiv.org [2022-10-23] Yunlong Cao, Fanchong Jian, ..., Xiaoliang Sunney Xie, October 04, 2022 link archive General
As winter inches closer, Dr. Fauci is sounding the alarm about a pair of “pretty troublesome” Covid variants.
The two descendants of omicron’s BA.5 subvariant, called BQ.1 and BQ.1.1, both have dangerous “qualities or characteristics that could evade some of the interventions we have,” Fauci told CBS News on Friday. The two sublineages are responsible for more than 10% of all current U.S. cases, according to the latest Centers for Disease Control and Prevention data — just one week after they weren’t even significant enough to list.
There’s no guarantee that the two strains will eventually overtake BA.5 as the dominant variant in the country. But if they do spread rapidly, they could threaten to reverse a nationwide decline in Covid cases, hospitalizations and deaths, leading Fauci to urge Americans against letting their guard down.
“As much as you want to feel good about the fact that cases are down, hospitalizations are down, we don’t want to declare victory too prematurely,” Fauci, the president’s chief medical adviser, said. “And that’s the reason why we’ve got to keep our eye out on these emerging variants.”
BA.5 still makes up nearly 68% of all current U.S. cases. The new strains are responsible for almost 20% of cases in a region that includes the New York City metropolitan area, which many experts consider the area a bellwether for Covid waves — due to its dense population and high volume of incoming international travelers.
Fauci said the strains have a concerning “doubling time,” referring to how quickly they spread. The U.K. Health Security Agency reported earlier this month that the strains even demonstrate a growth advantage over BA.5, which was considered the most contagious Covid strain to date.
BQ.1.1 is also particularly adept at dodging the protective antibodies you get from prior infection or vaccination, Fauci noted.
Scientists from Peking University in China published a study earlier this month that found BQ.1.1′s ability to evade antibodies was “far exceeding” that of BA.5. The study, which has yet to be peer-reviewed, also found that BQ.1.1 was capable of evading immunity from a previous BA.5 infection and some antibody drugs, including Bebtelovimab and Evusheld.
Still, the fact that both strains come from BA.5 means the new omicron-specific booster shots likely provide some protection against them. Early clinical trial data suggests that the boosters work well: Pfizer’s new shot generated a strong immune response against both omicron’s BA.4 and BA.5 subvariants, the company reported last week.
“The somewhat encouraging news is that it’s a BA.5 sublineage, so there are almost certainly going to be some cross-protection that you can boost up,” Fauci said.
Continued evolution of SARS-CoV-2 has led to the emergence of several new Omicron subvariants, including BQ.1, BQ. 1.1, BA.4.6, BF.7 and BA.2.75.2. Here we examine the neutralization resistance of these subvariants, as well as their ancestral BA.4/5, BA.2.75 and D614G variants, against sera from 3-dose vaccinated health care workers, hospitalized BA.1-wave patients, and BA.5-wave patients. We found enhanced neutralization resistance in all new subvariants, especially the BQ.1 and BQ.1.1 subvariants driven by a key N460K mutation, and to a lesser extent, R346T and K444T mutations, as well as the BA.2.75.2 subvariant driven largely by its F486S mutation. The BQ.1 and BQ.1.1 subvariants also exhibited enhanced fusogenicity and S processing dictated by the N460K mutation. Interestingly, the BA.2.75.2 subvariant saw an enhancement by the F486S mutation and a reduction by the D1199N mutation to its fusogenicity and S processing, resulting in minimal overall change. Molecular modelling revealed the mechanisms of receptor-binding and non-receptor binding monoclonal antibody-mediated immune evasion by R346T, K444T, F486S and D1199N mutations. Altogether, these findings shed light on the concerning evolution of newly emerging SARS-CoV-2 Omicron subvariants.
It is the vaccine & your continuance to vaccinate with sub-optimal non-neutralizing vaccine placing selection pressure not only on infectiousness, but viral VIRULANCE; will kill vulnerable & elderly
[...]
With these failed sub-optimal vaccines that are non-sterilizing, you are pressuring the infectiousness and virulence binding sites (epitopes) and causing a nightmare and we warned them over a year now to stop the vaccine. Stop! No new bivalent vaccine for already it is worthless. Stop the vaccine, it is worthless and it can create an evolutionary nightmare driving emergence of an infectious and lethal strain.
[...]
biorxiv.org [2022-10-31] Panke Qu, John P. Evans, ..., Shan-Lu Liu, October 20, 2022 link archive General
Omicron BA.5 has been the globally dominant SARS-CoV-2 variant and has demonstrated substantial neutralization escape compared with prior variants. Additional Omicron variants have recently emerged, including BA.4.6, BF.7, BA.2.75.2, and BQ.1.1, all of which have the Spike R346T mutation. In particular, BQ.1.1 has rapidly increased in frequency, and BA.5 has recently declined to less than half of viruses in the United States. Our data demonstrate that BA.2.75.2 and BQ.1.1 escape NAbs induced by infection and vaccination more effectively than BA.5. BQ.1.1 NAb titers were lower than BA.5 NAb titers by a factor of 7 in two cohorts of individuals who received the monovalent or bivalent mRNA vaccine boosters. These findings provide the immunologic context for the rapid increase in BQ.1.1 prevalence in regions where BA.5 is dominant and have implications for both vaccine immunity and natural immunity.
Again, we warn that it is the mRNA antigenic-specific, high-affinity, vaccinal antibodies that are binding to the virus spike antigen yet not neutralizing the virus (stopping infection or replication or transmission and actually enhancing replication) and driving the natural selection of more infectious sub-variants. When you vaccinate (roll out a vaccine) across all age groups into a pandemic with ongoing elevated infectious pressure and using a non-sterilizing, non-neutralizing vaccine, then selection pressure will drive selection and emergence of more ‘fitter’ variants and some (one) can even be ‘hotter’ (more virulent in terms of causing severity of illness). CVB warns openly about this and IMO, this is a smart scientist, learned, pay attention to him.
biorxiv.org [2022-11-11] Jessica Miller, Nicole P. Hachmann, Ai-ris Y. Collier, Ninaad Lasrado, Camille R. Mazurek, Robert C. Patio, Olivia Powers, Nehalee Surve, James Theiler, Bette Korber, Dan H. Barouch, November 02, 2022 link archive General
New offshoots of the Omicron Covid-19 variant that virus experts say appear to spread easily are on the rise in the U.S., the latest federal data show, underscoring how the virus is mutating and presenting new risks as it proliferates.
Two of the Omicron subvariants, both related to the BA.5 version that drove the most recent U.S. surge, are called BQ.1 and BQ.1.1. They were estimated to represent a combined 11.4% of U.S. Covid-19 cases by mid-October, according to estimates the Centers for Disease Control and Prevention released Friday.
[...]
wsj.com [2022-11-24] Jon Kamp, Brianna Abbott, October 14, 2022 link archive General
BQ.1, BQ.1.1, XBB, and XBB.1 are the most resistant SARS-CoV-2 variants to date
Serum neutralization was markedly reduced, including with the bivalent booster
All clinical monoclonal antibodies were rendered inactive against these variants
The ACE2 affinity of these variants were similar to their parental strains
Summary
The BQ and XBB subvariants of SARS-CoV-2 Omicron are now rapidly expanding, possibly due to altered antibody evasion properties deriving from their additional spike mutations. Here, we report that neutralization of BQ.1, BQ.1.1, XBB, and XBB.1 by sera from vaccinees and infected persons was markedly impaired, including sera from individuals boosted with a WA1/BA.5 bivalent mRNA vaccine. Titers against BQ and XBB subvariants were lower by 13-81-fold and 66-155-fold, respectively, far beyond what had been observed to date. Monoclonal antibodies capable of neutralizing the original Omicron variant were largely inactive against these new subvariants, and the responsible individual spike mutations were identified. These subvariants were found to have similar ACE2-binding affinities as their predecessors. Together, our findings indicate that BQ and XBB subvariants present serious threats to current COVID-19 vaccines, render inactive all authorized antibodies, and may have gained dominance in the population because of their advantage in evading antibodies.
cell.com [2022-12-18] Qian Wang, Sho Iketani, ..., David D. Ho, December 13, 2022 link archive General
Over the past three years, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has repeatedly experienced pandemics, generating various mutated variants ranging from Alpha to Omicron. In this study, we aimed to clarify the evolutionary processes leading to the formation of SARS-CoV-2 Omicron variants, focusing on Omicron variants with many amino acid mutations in the spike protein among SARS-CoV-2 isolates. To determine the order in which the mutations leading to the formation of the SARS-CoV-2 Omicron variants, we compared the sequences of 129 Omicron BA.1-related isolates, 141 BA.1.1-related isolates, and 122 BA.2-related isolates, and tried to dissolve the evolutionary processes of the SARS-CoV-2 Omicron variants, including the order of mutations leading to the formation of the SARS-CoV-2 Omicron variants and the occurrence of homologous recombination. As a result, we concluded that the formations of a part of Omicron isolates BA.1, BA.1.1, and BA.2 were not the products of genome evolution as is commonly observed in nature, such as the accumulation of mutations and homologous recombinations. Furthermore, the study of 35 recombinant isolates of Omicron variants BA.1 and BA.2, confirmed that Omicron variants were already present in 2020. The analysis we have shown here is that the Omicron variants are formed by an entirely new mechanism that cannot be explained by previous biology, and knowing the way how the SARS-CoV-2 variants were formed prompts a reconsideration of the SARS-CoV-2 pandemic.
Comprehensive panels of "reversion mutations" found in general circulation look like an experiment
On August 5th 2023 a Japanese research team published a pre-print that appears to contain the most important and shocking revelations of the covid era.
Atsuki Tanaka and Takayuki Miyazawa, of Osaka Medical University and Kyoto University, wanted to trace the historical evolution of the omicron variant of SARS-CoV2 by studying viral sequences found "in the wild" and deposited in public databases.
In doing this they found around 100 separate omicron subvariants that could not conceivably have arisen through natural processes. The existence of these variants seems to provide definitive proof of large-scale lab creation and release of covid viruses.
Moreover the variants appear to form comprehensive panels of mutations typical of those used in "reverse genetics" experiments to systematically test the properties of different parts of viruses.
The authors also found exact matches to omicron variants in sequences originating from Puerto Rico which were deposited in databases in 2020 - over a year before the announcement of the discovery of omicron in South Africa.
Coupled with observations of implausibly low numbers of "silent" mutations in SARS-CoV2 variants, Tanaka and Miyazawa argue that all variants emerging since the original Wuhan outbreak are unnatural, and speculate that they represent an experimental program to test determinants of the infectivity and pathogenicity of SARS-CoV2 in the global population.
[...]
zenodo.org [2023-08-10] Tanaka, Atsushi; Miyazawa, Takayuki, August 5, 2023 link archive General
While the DOE, FBI, and CIA all now back the possibility of a lab leak pandemic scenario, a new study by Japanese researchers sheds light on the genetic investigation. Appearing to show human intervention in the creation of the Omicron variant, scientists may now be forced to factor synthetic creation into the discussion.
Japanese researcher, Dr. Takayuki Miyazawa, took to the streets of Japan in an historic effort to convey information about research showing the Omicron variant may have been artificially synthesized. Learn how The HighWire has been leading the worldwide media coverage of this important issue.
References:
Unnaturalness in the evolution process of the SARS-CoV-2 variants and the possibility of deliberate natural selection
As the world still comes to grips with coronavirus’ variant, said to be highly transmissible if not deadlier than the Delta variant, that has dimmed the chances of a pandemic-free 2022, a fresh surge in US and Europe is now being blamed on a combination of the two.
Delmicron, a combination of the virus’ Delta and Omicron variants, can transmit even faster. While Covid-19 infections only involve a single mutant strain, two can strike simultaneously in extremely rare cases.
[...]
financialexpress.com [2022-01-03] December 28, 2021 link archive General
Viruses are programmed to mutate and variants are bound to emerge. So is the case with the SARs-COV-2 virus. Since the onset of the novel coronavirus in early 2020 up until now, new COVID-19 variants have cropped up time and again.
With the latest coronavirus variant Omicron, wreaking a lot of havoc around the world, scientists now warn against the emergence of a new threat termed as 'Delmicron'. Reports suggest that the rise in the number of COVID-19 cases in the west has been caused by a mix of Delta and Omicron variants, hence the name 'Delmicron'.
However, it is yet to be seen whether the new wave of infections will be worse than the impact of Omicron or if it could pose more dangers to the most vulnerable. Let us find out.
[...]
timesofindia.indiatimes.com [2022-01-03] Dec 31, 2021 link archive General
Scientists in Cyprus have claimed they have discovered a COVID-19 variant that combines Delta and Omicron, dubbing it “Deltacron” – but experts quickly dismissed the claim and blamed the finding on contamination, according to reports.
Leondios Kostrikis, professor of biological sciences at the University of Cyprus, and his team identified 25 cases of the hybrid strain, which they named “Deltacron” due to Omicron-like markers in the Delta genomes, Bloomberg News reported.
“There are currently Omicron and Delta co-infections and we found this strain that is a combination of these two,” Kostrikis told Sigma TV, according to Bloomberg.
Birthing mother diagnosed with both coronavirus and influenza virus infection simultaneously; health officials estimate many other patients also came down with both pathogens but have not been diagnosed
Israel has documented its first case of the so-called "flurona" — a simultaneous coronavirus and influenza virus infection, Ynet has learned on Thursday.
The double infection was first identified in a woman who went into labor this week at Rabin Medical Center in Petah Tikva. According to the hospital, the young mother, who is not vaccinated against either pathogen, is feeling well and is expected to be discharged from the hospital later Thursday.
[...]
ynetnews.com [2022-01-03] Adir Yanko, 12.30.21 link archive General
At a time when the world is grappling with Delta and Omicron variants, and the combination of both called ‘Delmicron’ variant of coronavirus, Israel has reported its first case of 'flurona'— a simultaneous coronavirus and flu infection.
The first 'flurona' virus was found in a woman who recently gave birth in a hospital in Petah Tikva city, in central Israel, Ynet news portal reported on Thursday.
The young woman, a patient in Beilinson Hospital in Petach Tikva., was unvaccinated and results from the hospital detected the co-presence of both the flu and the Covid 19 pathogens
mirror.co.uk [2022-01-03] By Leigh Mcmanus, 31 Dec 2021 link archive General
The pace at which XBB.1.5 is (has) supplanting (supplanted) BA.5 and BQ.1.1 etc. is staggering.
They have designed the roll-out, the vaccine, all of it to never end; Fauci, Bourla, Bancel, Francis Collins, Walensky, CDC, NIH, FDA et al., they all know that as long you mass vaccinate across all age-groups and keep injecting while there is massive circulating virus, using a gene injection (vaccine) that does not sterilize (neutralize) the virus (stop infection or transmission), then natural selection pressure will select for the fittest, most infectious variants that could overcome that sub-optimal pressure, become enriched in the environment, and go on to become the new dominant sub-variant, case in point, XBB.1.5. There will be viral immune escape, original antigenic sin, and antibody-dependent enhancement of infection (and/or disease), as well as now emerging indications of immune tolerance (based on IgG4 class switching).
[...]
palexander.substack.com [2022-12-31] Dr. Paul Alexander, December 31, 2022 link archive General
A new omicron subvariant that fuses two prior subvariants from the wildly contagious strain that first emerged in South Africa is spreading rapidly in the northeastern United States, CDC data shows
A new most transmissible-yet COVID variant has established dominance in the New York area, fueling rising infection rates across the five boroughs as a looming nurses' strike and ongoing concerns about RSV in kids stoke fresh anxiety about the years-long pandemic.
That XBB.1.5 strain, another omicron descendant, is a highly contagious "recombinant" one spawned from two prior, and different omicron subvariants. Those two were considered more transmissible than their predecessors at the time they emerged, and the resulting fusion -- XBB.1.5 -- is believed to be that much more potent in terms of infectiousness.
At this point, the World Health Organization doesn't have any data to indicate it is more lethal or causes more severe cases, but the rate at which it is spreading, especially in the northeastern United States, is raising some questions.
"It is the most transmissible subvariant that has been detected yet," she told reporters this week. "The more this virus circulates, the more opportunities it will have to change."
And nowhere is XBB.1.5 circulating faster than the northeast, according to CDC data. Its latest update estimates the variant's prevalence in the New York region, which also encompasses New Jersey, Puerto Rico and the Virgin Islands, to be 72.2% but as high as 80.8%, compared with a 40.5% estimated prevalence and 61% high at the national level.
[...]
nbcnewyork.com [2023-01-07] Jennifer Millman, Jan 5, 2023 link archive General
A new offshoot of the Covid-19 Omicron variant is taking over in parts of theU.S., especially in the Northeast, amid signs of rising infection numbers after the winter holidays.
Virus experts and doctors say a combination of holiday gatherings and the arrival of the XBB.1.5 subvariant is causing more Covid-19 infections, as reflected in rising hospitalization numbers and a recent climb in wastewater virus levels.
[...]
wsj.com [2023-01-08] Jon Kamp, Brianna Abbott, January 6, 2023 link archive General
The World Health Organization said the omicron XBB.1.5 variant does not have any mutations known to make people sicker but that it needs more real-world data to draw conclusions about its severity.
The WHO said XBB.1.5 is one of the Covid subvariants that is most adept at dodging immunity.
The global health agency said the subvariant could cause cases to rise globally, though it needs more data from countries other than the U.S.
[...]
cnbc.com [2023-01-13] Spencer Kimball, January 11, 2023 link archive General
Our data show that the BQ.1.1 and XBB.1 variants escaped neutralizing antibodies substantially more effectively than the BA.5 variant by factors of 7 and 17, respectively, after monovalent mRNA boosting and by factors of 7 and 21, respectively, after bivalent mRNA boosting. The neutralizing antibody titers to BQ.1.1 and XBB.1 were dramatically lower than titers to the WA1/2020 strain by factors of 53 and 127, respectively, in the monovalent booster cohort and by factors of 80 and 232, respectively, in the bivalent booster cohort. These findings suggest that the BQ.1.1 and XBB.1 variants may reduce the efficacy of current mRNA vaccines and that vaccine protection against severe disease with these variants may depend on CD8 T-cell responses.5 The higher neutralizing antibody titers against omicron variants after monovalent mRNA boosting in the 2022 cohort than in the 2021 cohort probably reflect the greater numbers of vaccine doses and infections in the 2022 cohort. The incorporation of the R346T mutation into multiple new SARS-CoV-2 variants suggests convergent evolution.
These subvariants have learned to escape the antibodies from the bivalent vaccines with great alacrity over a short period of time. In a letter from Miller et al, the authors concede that the bivalent boosters in theory are essentially useless against the newer subvariants.
nejm.org [2023-01-19] Jessica Miller, Nicole P. Hachmann, ..., James Theiler, ..., Dan H. Barouch, January 18, 2023 link archive General
Six cases in four countries have been detected since late July. Scientists are keeping an eye on the new lineage, named BA.2.86, because it has 36 mutations that distinguish it from the currently-dominant XBB.1.5 variant.
So far there is no evidence that BA.2.86 spreads faster or causes more serious illness than previous versions. The CDC said its advice on protecting yourself from COVID remains the same.
What is new about COVID?
COVID infections and hospitalizations have been rising in the U.S., Europe and Asia, with more cases in recent months attributed to the EG.5 "Eris" subvariant, a descendant of the Omicron lineage that originally emerged in November 2021.
Over the past few days, public health authorities have documented one case each of BA.2.86 in the United States, the UK, and Israel, and three cases in Denmark.
What do scientists say about BA.2.86?
BA.2.86 stems from an "earlier branch" of the coronavirus, so it differs from the variant targeted by current vaccines, explained Dr. S. Wesley Long, medical director of diagnostic microbiology at Houston Methodist Hospital.
He said it remains to be seen whether BA.2.86 will be able to out-compete other strains of the virus or have any advantage in escaping immune responses from prior infection or vaccination.
But many countries have drastically reduced testing of patients and their efforts to analyze the genomes of the viruses causing new COVID cases. In that situation, the trajectory of BA.2.86 "doesn't look good right now," given the speed at which new cases are being identified, said Dr. Eric Topol, a genomics expert and director of the Scripps Research Translational Institute in La Jolla, California.
[...]
See related data element: ☕️ LOCKDOWN 2023? ☙ Sunday, August 20, 2023 ☙ C&C NEWS ?
reuters.com [2023-08-21] Deena Beasley, Nancy Lapid, August 19, 2023 link archive General
Eris – the most recent “Covid variant” – is supposedly causing spikes in cases all over the world. The story goes that England, Ireland and US are all being hit hard, it’s reached Australia too.
In yet another blow to the “BRICS will save us” crowd, India and China are playing along.
We’ve already been over everything you need to know about “Eris” here. Long story short, “Covid” is just another made up name for the flu, and the “variants” are coats of paint they slap on the narrative to try and keep it looking fresh.
In that same article I theorised Eris’ existence was a need to keep Covid alive, and that is part of it…but I also missed something obvious: The next round of Covid “vaccines” hits the shelves next month.
For those who have lost count, I think we’re up to six or seven shots now.
This “updated vaccine” is nothing to do with Eris, of course, as much as the language in the headlines implies it’s been “adapted” for the latest variant, it hasn’t. It was in the works before Eris was even said to exist.
Moderna had the brass neck to claim that they did a “trial” showing their updated vaccine protects against Eris. Considering Eris first hit the headlines just a few weeks ago it looks like Moderna may have broken their own record in terms of speedy “trials”.
It’s just the same old slop it always was.
Hell, let’s be honest, it could be water. It could be ANYTHING.
The content of the syringe was never the important part. After all, what you were being injected with wasn’t the point, the point was that you got injected because they told you to.
It was about forcing obedience, setting the vaccine mandate precedent and seeing how effectively people could be gaslit into taking a shot that they’d already been told they don’t need and doesn’t work.
Well, that and governments handing over VAST amounts of cash to pharmaceutical companies, obviously.
But they already have the money, and most people (allegedly) took the vaccine…so why are they still going?
You have to appreciate the huge amount of effort that went into hypnotizing millions – maybe billions – of people into acting against their own best interests, it’s a spell that’s easier to maintain than restart. If they start letting people forget, then soon they’ll have to begin the ritual all over again.
And the magic is already wearing off.
Consider that, allegedly, over 200 million Americans took the first dose in 2021, and that by the time boosters were coming out in the fall of 2022 it was down to 50 million. That’s a 75% drop-off in only a year.
The power is slipping away, and as they scramble to get it back you can probably expect “Eris” to get a lot worse.
off-guardian.org [2023-08-21] Aug 18, 2023 link archive General
The U.S. Centers for Disease Control and Prevention (CDC) stated on Aug. 23 that the new BA.2.86 COVID-19 lineage may cause infection in people who received vaccines or previously had the virus.
The CDC stated that it’s too soon to know whether this might cause more severe illness than previous variants. But because of the high number of mutations detected in this lineage, there are concerns about the effectiveness of immunity from vaccines and previous infections, according to the agency.
“The large number of mutations in this variant raises concerns of greater escape from existing immunity from vaccines and previous infections compared with other recent variants,” the CDC stated in its assessment. “For example, one analysis of mutations suggests the difference may be as large as or greater than that between BA.2 and XBB.1.5, which circulated nearly a year apart.”
But it also stated that “virus samples are not yet broadly available for more reliable laboratory testing of antibodies, and it is too soon to know the real-world impacts on immunity.”
The agency noted that it detected at least two cases with the BA.2.86 variant in the United States, although few other details were provided. It was also found in Israel, the UK, South Africa, and Denmark.
One of the BA.2.86 cases was found in a person detected via the CDC’s traveler surveillance system, while it noted that cases being found in several countries is evidence of international transmission.
“Notably, the amount of genomic sequencing of SARS-CoV-2 globally has declined substantially from previous years, meaning more variants may emerge and spread undetected for longer periods of time,” the assessment reads. “It is also important to note that the current increase in hospitalizations in the United States is not likely driven by the BA.2.86 variant. This assessment may change as additional data become available.”
The CDC noted that most of the U.S. population has COVID-19 antibodies from a previous infection, vaccination, or both and stated that it’s likely that the antibodies will provide some protection against the variant.
The agency stated on Aug. 23 that the slight recent increase in hospitalizations in the United States isn’t likely driven by the BA.2.86 lineage.
[...]
theepochtimes.com [2023-08-26] Jack Phillips, Aug 23 2023 link archive General
The primary cause of death is defined as the condition, injury, disease, situation or event that initiated the chain of events resulting in a person’s death.
Weekly COVID-19 deaths are at their lowest numbers since March 2020, according to CDC data.
Experts are linking a new COVID-19 variant, nicknamed "Eris," to a recent spike in cases throughout the country.
In Connecticut, Center for Disease Control and Prevention (CDC) data from Aug. 12 shows 161 new COVID-19 hospitalizations compared to 118 the previous week.
“It is not necessarily more dangerous than the previous variants, but we are seeing an uptick associated with that,” said Dr. Ulysses Wu, chief epidemiologist for Hartford HealthCare.
Then, there’s the new BA.2.86 variant that has caught experts’ attention. So far, CDC reports show just two cases in the entire United States, but as of last week, the variant is being monitored for its increased ability to evade the immune system.
“I don’t want people to panic when they hear that. It’s not necessarily that your immune system can’t take care of it, it just means that if you’ve been exposed to COVID in the past, or if you’ve gotten a vaccination, your immune system may not recognize this new variant,” Wu said.
[...]
msn.com [2023-08-31] Dave Peck, August 29, 2023 link archive General
Pirola is a strain of COVID-19 first reported in August of 2023. As of August 19th, only seven cases have been reported to the Centers for Disease Control and Prevention (CDC).
Pirola represents an entirely new lineage of COVID-19, meaning it isn't derived from a previous variant, such as Omicron. Pirola has 30 mutations, which is more mutations than other variants currently circulating. This means that current vaccinations—as well as the one rolling out this fall—may not protect against Pirola as well as Omicron variants, for which the vaccination was designed. That said, it’s feasible that high population-level immunity may prevent an Omicron-like surge, according to Dr. Rajendram Rajnarayanan, Assistant Dean of Research and Associate Professor at the New York Institute of Technology College of Osteopathic Medicine at Arkansas State University.
[...]
reviewed.usatoday.com [2023-08-31] Kaleb A. Brown, August 30, 2023 link archive General
A friend asked for my opinion about a story that was just published. Rather than provide only him with an answer, I figured that others might benefit from the insights of a viral immunologist who specializes in vaccinology, and that has been on the front lines of COVID-19 science since the beginning. Here is my take…
The story was given the title “This Fall's Covid Variant Might Really Be Different“.
It could just as easily have been entitled “This Fall's Covid Variant Might Not Be Different in Any Meaningful Way“.
“BA.2.86—dubbed “pirola” […] has been detected in only about a dozen people but it has surfaced in all corners of the world.“
BA.2.86, also known as ‘pirola’ (named after an asteroid near the planet Venus), is the newest variant of SARS-CoV-2 (the causative agent of the disease we call ‘COVID-19’). This new variant is ‘under monitoring’.
This quote from the paper suggests that the virus is not highly transmissible and/or it is not particularly dangerous. A highly transmissible virus that is in 12 people sprinkled around the world would be capable of spreading rapidly. I suspect that it has likely spread much more than what is currently appreciated, but it is not causing substantial disease, so nobody really cares enough to get tested. A dangerous virus would be easily detected and would prompt testing because it would be causing severe disease and death, which could not be missed. This sentence alone alleviates concerns about this variant of SARS-CoV-2.
“What’s troubling about this variant, scientists say, is that it contains more than 30 mutations on the spike protein, which is what helps the virus enter cells and cause an infection. This means it might be able to evade current vaccines and previous infections more easily, and it likely won’t be a great match with the fall booster expected to be approved soon.“
An accumulation of mutations in the spike protein are exactly what we would expect. After all, the COVID-19 shots only target the spike protein. It is one of the poor design features of these shots. The COVID-19 shots do not come anywhere close to conferring immunity against infection with nor transmission of SARS-CoV-2. Applying a non-lethal selective pressure against a single protein from a virus is the perfect recipe for promoting the emergence of naturally occurring variants that have changed the target protein enough to facilitate long-term survival of the virus.
Of course new variants will be better able to escape historical immunity. However, the reporter failed to disseminate important information here. Naturally acquired immunity is superior to the sub-par immune responses induced by outdated COVID-19 shots. Importantly, naturally acquired immune responses target multiple components of SARS-CoV-2, not just the spike protein. A person with naturally acquired immunity will have both antibodies and T cells that can kill SARS-CoV-2 by virtue of recognizing things other than the spike protein. So, it will be more difficult for new variants to completely evade naturally acquired immunity. It would be expected that those who only have had immune responses induced by the COVID-19 shots will be more susceptible to getting infected and will be prone to more severe illness than people with naturally acquired immunity.
Also, this cycle of ever-emerging new variants of a virus is not new. It occurs with every cold-causing virus. People get infected, mount an effective immune response and then are protected until the virus has changed enough to cause mild disease again. This has been happening our entire lives. With pathogens that are not particularly serious, they key is to not allow your immunity to get outdated by isolating yourself from the microbial world. This is likely a key reason why many people, especially children, got so sick with so many pathogens once they were released from their long-term COVID-19 lockdown prisons.
Another point missed in the article is that too many mutations in the protein that is needed for a virus to infect cells can lead to reduced infectivity, making it less transmissible and less dangerous.
[...]
New strains of viruses do not pop out of nowhere. More likely, they are derived from biological systems that are exerting non-lethal selective pressures on them. At the top of this list are those whose immune responses against SARS-CoV-2 were induced only via COVID-19 shots. If you want to slow the emergence of new variants, STOP THE SHOTS! Stop putting those of us who know better at risk of getting exposed to a genuinely very dangerous version of SARS-CoV-2. Similarly, stop manufacturing viruses like SARS-CoV-2 in labs; they have not gone through the same selective pressures that naturally occurring viruses have.
“Lessler says the fact that the locations where the variant has been identified haven’t experienced large surges in cases is a hopeful sign that the strain might not be proliferating rapidly.”
I agree. There are much more concerning medical issues to tackle.
““But that doesn’t mean it can’t mutate to be able to spread quickly at some point,” he notes.“
So many ‘experts’ want to keep their finger near the ‘fear trigger’. An equally valid way of stating this is, “But that doesn’t mean it can’t mutate to be even less capable of spreading at some point“. If we really want to reduce the chance of dangerous mutations occurring in SARS-CoV-2, STOP THE SHOTS!
In closing, my expert opinion matches that of Dr. David Dowdy…
“Some public health experts caution against reading too much into the new variant.
“We don’t want to be sounding alarm bells over a variant that is just as likely to die out as it is to become the next big thing,” says David Dowdy, a professor of epidemiology at Johns Hopkins Bloomberg School of Public Health. “If we did that for every single variant we’d be sounding alarm bells every single day.”“
This kind of logic seems rare these days and is so very welcome. I couldn’t agree more.
viralimmunologist.substack.com [2023-09-01] Dr. Byram W. Bridle, August 30, 2023 link archive General
? It’s been a while since we got to watch a good variant horror movie. But now, according to people on our side, this could be finally it, the depopulation event. Let’s review the evidence and figure out: how concerned should we be?
Amongst this year’s ever-spreading alphabet soup of overcooked numbers and letters, there is finally something to talk about: JN.1, the latest mutation to spring out of Pirola’s trousers, which lineage was originally birthed from Omicron, which helpfully tends to loiter in the upper respiratory system and rarely ventures down into the lungs. Due to the J and the N, I call the new variant ‘Pirola Junior.’
Let’s begin by noting that corporate media has found little to worry about as Pirola Junior edges out the others to become a sort of red-nosed Rudolph leading the pack of variants. On Tuesday, Reuters reported that the WHO labeled the new strain a “variant of interest,” but dumped cold water on the story right in the headline:
Pirola Junior is, of course, being called “even more infectious” than the nineteen previous “super infectious” covid variants. They say — and I am not making this up — Pirola Junior is four hundred times more infectious than the original Wuhan strain. Apparently infection ability is potentially infinite; there’s no upper limit. In other words, it can now infect you through a concrete wall using bluetooth.
The new variant seems busier in Europe. From Bloomberg, yesterday:
I don’t know whether “1 in 24” sounds like a lot or not, but applying mathematics (and the calculator on my phone) that is about four percent. Most people have mild symptoms. Hospitalizations are increasing but remain below last year’s December peak. And, here in the U.S., apparently we’re just now getting around to throwing out all the leftover PPE from the last pandemic panic. From Bloomberg, Wednesday:
Notwithstanding all the good signs, the panic police remain unsatisfied. For example, take (and please keep) hysterical covid fearmonger Eric Fingle-Dingle, who is hysterically fearmongering again. His take on JN.1, yesterday, was an urgent call for more masking:
Yawn. So far we have an unremarkable covid variant, disinterested corporate media, and below-average (albeit increasing) hospitalization levels. So what gives? What’s stirring up all the natives down at the Fauci Memorial Reservation this time?
Two data fuel all the delirious trepidation. First, the vaccines are completely useless against the heavily-mutated Pirola variant (that is, if they ever accomplished anything in the first place). More relevant, for some reason people without fully functioning immune systems lack good biological defenses to the new variant. But nobody’s really talking about this issue, as you can imagine.
More discussed is the second fact fueling the social media chatter: the rateof increase of JN.1 hospitalizations. It’s really the only JN.1 figure worth mentioning. Reported hospitalizations are low but rising rapidly, or “surging.” That’s rattled covid maniacs like Eric Dingleberry MD, who is generally unremarkable, repetitive, and boring, but the rapid increase over a few days has caused chronic heterodox doomcryer Geert Vanden Bossche (who I respect but take with a grain of salt) to prophesy that this is the big one:
In the clip, to prove he is right, Geert asked himself several apocalyptic questions and then provided his own answers:
Will the chain of more and more infectious variants ever stop? Yes. We will not have yet another simply more infectious variant that will displace JN.1.
Will a completely new, highly-virulent variant emerge in highly-vaccinated countries? Yes.
Will the rate of mortality and morbidity start to exponentially increase? Yes — but only in the vaccinated. It will be difficult to get these figures though.
Will Unvaccinated or people in low-uptake Africa be affected? No.
In short, Geert predicts that JN.1 is the end of the line for mild but more infectious variants. He thinks that the next variant will be super-deadly — but only to vaccinated folks. (In a different interview, someone pressed him for a mortality figure and Geert reluctantly estimated 30-40%.) Yesterday Geert published his new theory in a dense, technical Substack, which can be summarized using his own words (lightly edited):
The Omicron descendants, bred in highly C-19 vaccinated populations, have transformed a naturally occurring pandemic into an 'inescapable immune escape pandemic' through the generation of significant immune selection pressure and immune refocusing. The SC-2 variant JN.1 is now rapidly outpacing other co-circulating variants. While the rapidly spreading JN.1 variant does not evoke concerns about increased intrinsic virulence, its widespread dominance is of high concern. The presence of additional, productivity-enhancing mutations in viral proteins other than the S protein indicates the exertion of immune selection pressure … strongly suggests a reduction in the production of virulence-inhibiting antibodies.
I can’t argue with Geert’s science. Literally I couldn’t argue with him. He’s way out of my scientific league. But I do not yet see the evidence for his theory. From day one I asked public health officials about antibody-dependent enhancement and immune escape and never once got any intelligent answer, not one time. I’ve since learned why. Most public health officials don’t understand vaccine science; they’re just good liars who can repeat whatever they’re told in a strong, confident tone of voice.
Their smug, arrogant condescension toward anyone who questions them is just an act. Scientists didn’t refuse to answer questions because they actually believed they’re better than us and didn’t want to sully themselves with “conspiracy theories.” The real reason is that, if they started trying to answer questions, it would have quickly become obvious they had no idea what they’re talking about.
Geert knows what he’s talking about. I’d take Geert over a CDC official any day. And his predictions have been right before. Geert was 100% right with his prediction that mass vaccination would drive evolution of a large number of immune escape variants.
The plain evidence shows an unusual number of major covid mutations all trending toward evading vaccine coverage.
But his worst-case scenarios have yet to emerge. There is solid evidence that the vaccines can degrade immune systems, cause catastrophic autoimmune problems, and enhance some folks susceptibility to common (and uncommon) infections. But — and this is the critical part — besides anecdotally witnessing many of our jabbed friends and relatives having chronic coughs and getting repeated (mild) covid infections, there is no evidence of serious systemic immune failures in large numbers.
Geert might be right. And it’s not like we have a lot of options for who to believe. Even with fabulously-expensive satellite-mounted telescopes, no intelligent thought can be detected at the government-funded health agencies. But Geert’s theory depends on a new, as-yet-unseen variant that would violate evolutionary norms.
See, viruses are under constant pressure to mutate to be lessvirulent and more transmissible, which is exactly what we’ve seen with Pirola and prior covid variants. A virus that kills people or keeps them in bed does not survive better than a milder virus that lets folks move around and spread the germ.
The bottom line? So far, Pirola Junior appears to be yet another milder, ever-more-infectious covid variant. But I’ll keep an eye on things for you and let you know immediately if any evidence supporting Geert’s prediction evolves. Till then, don’t take your medical advice from Eric Fingle-de-Dee, MD.
coffeeandcovid.com [2023-12-23] Jeff Childers, December 22, 2023 link archive General
I’m sure you remember the Omicron variant (BA.1), which was dominant for about 2-3 months between 2021 and 2022. That seems to be the normal period before a new variant takes over. Most variants disappear faster than that. We’re soon reaching the benchmark dominance period with JN.1, and so far, the variant doesn’t show any sign of slowing down. Just the opposite:
The cited recent Lancet study described JN.1 as having the greatest ‘immune escape’ of any variant so far. Immune escape refers to a variant’s ability to ignore whatever marginal, temporary “protection” the mRNA jabs offer:
Particularly notable was the finding that JN.1 strongly resisted the XBB.1.5 vaccine, making it one of the most immune-evading variants discovered so far, according to the researchers.
On the plus side, JN.1 is not reported to be causing more severe infections, so it does not seem more virulent. What are you all seeing anecdotally?
Mercifully, corporate media has gotten bored with it and stopped pushing covid news all the time, so we have to dig around a little when we want to know what is going on. Here’s my conclusion: There’s no reason to panic, but Geert’s ‘final variant’ prediction has not yet been disproved and remains viable. I’ll keep monitoring the situation.
coffeeandcovid.com [2024-02-14] Jeff Childers, February 13, 2024 link archive General
Since the earliest days of the pandemic, there has been one collective goal for bringing it to an end: achieving herd immunity. That’s when so many people are immune to a virus that it runs out of potential hosts to infect, causing an outbreak to sputter out.
Many Americans embraced the novel farmyard phrase, and with it, the projection that once 70% to 80% or 85% of the population was vaccinated against COVID-19, the virus would go away and the pandemic would be over.
Now the herd is restless. And experts at the Centers for Disease Control and Prevention have set aside herd immunity as a national goal.
An Emergency Use Authorization (EUA) is a mechanism to facilitate the availability and use of medical countermeasures, including vaccines, during public health emergencies, such as the current COVID-19 pandemic. Under an EUA, FDA may allow the use of unapproved medical products, or unapproved uses of approved medical products in an emergency to diagnose, treat, or prevent serious or life-threatening diseases or conditions when certain statutory criteria have been met, including that there are no adequate, approved, and available alternatives. Taking into consideration input from the FDA, manufacturers decide whether and when to submit an EUA request to FDA.
US Rep Kurt Schrader of Oregon presses Dr. Fauci on development times and effectiveness of vaccines. According to Dr. Fauci:
Average time to develop a vaccine is about 7 years.
The fastest a vaccine has ever been developed was about a year and a half, which was for the Zika virus and which never came to full fruition because the Zika "kinda disappeared."
There are more failures than successes in developing vaccines.
Schrader: "What's the probability that a vaccine comes to market?"
Fauci: "There are more failures than there are successes."
Shrader: "About 6%."
Fauci: "Right."
According to Fauci, "All RNA viruses mutate, that doesn't mean they change."
youtu.be [2020-07-02] NowThis News YT channel, Jun 23, 2020 link archive General
More information on Coronavirus vaccines, adverse reactions, mandatory policies, etc.
I found the Pearson correlation coefficient between the proportion of people who have received a booster dose and the respective average weekly excess mortality of each state to be 0.63, which is known as a strong correlation.
The 2 states with the lowest excess mortality for 2022 (Sachsen and Thüringen) are the ones with the lowest booster rates.
Boosters are causing excess mortality by making people more susceptible to severe COVID-19 which I deduce from the following observations:
Each of the 3 waves of booster administrations is followed by a wave of COVID-19 cases 13 weeks later and a wave of excess mortality 15-16 weeks later.
VAERS reports show a peak in reports about COVID-19 pneumonia in the 14th week after administration of a booster dose.
The Pearson correlation between the average weekly excess mortality rate of 2022 and the proportion of people who have received a booster is 0.63 (strong).
The 2 states with the lowest excess mortality rates are the ones with the lowest booster rates.
Extended booster vaccination has been shown to induce humoral and cellular immune tolerance in mice.
[...]
vigilance.pervaers.com [2022-12-28] Fabian Spieker, December 23, 2022 link archive General
Prof. Mattias Desmet joins Dr. Reiner Fuellmich and the Stiftung Corona Ausschuss (Investigative Corona Committee) to discuss why so many, otherwise highly intelligent people, seem to be so easily deceived by the main-stream narrative of the COVID-19 pandemic. [Note: Discussion with Prof. Desmet starts at about the 3:26:00 mark and is in English. The concept of "Mass Formation Psychosis" is discussed and perceived to be what is being witnessed around the world regarding the willingness of people to accept official COVID-19 policies, even though they logically do not make sense.]
In this video we are going to explore the most dangerous of all psychic epidemics, the mass psychosis. A mass psychosis is an epidemic of madness and it occurs when a large portion of a society loses touch with reality and descends into delusions. Such a phenomenon is not a thing of fiction. Two examples of mass psychoses are the American and European witch hunts 16th and 17th centuries and the rise of totalitarianism in the 20th century.
This video will aim to answer questions surrounding mass psychosis: What is it? How does is start? Has it happened before? Are we experiencing one right now? And if so, how can the stages of a mass psychosis be reversed?
Dr. Robert Malone, inventor of the mRNA vaccine, breaks down the "mass formation" phenomenon that makes it difficult to reason with those who have fallen victim to the globalist leader propaganda. Hear what he says is the hope we have before a total takeover.
Scientists on a committee that encouraged the use of fear to control people’s behaviour during the Covid pandemic have admitted its work was “unethical” and “totalitarian”.
Members of the Scientific Pandemic Influenza Group on Behaviour (SPI-B) expressed regret about the tactics in a new book about the role of psychology in the Government’s Covid-19 response.
SPI-B warned in March last year that ministers needed to increase “the perceived level of personal threat” from Covid-19 because “a substantial number of people still do not feel sufficiently personally threatened”.
Gavin Morgan, a psychologist on the team, said: “Clearly, using fear as a means of control is not ethical. Using fear smacks of totalitarianism. It’s not an ethical stance for any modern government. By nature I am an optimistic person, but all this has given me a more pessimistic view of people.”
Mr Morgan spoke to author Laura Dodsworth, who has spent a year investigating the Government’s tactics for her book A State of Fear, published on Monday.
In his 1921 book on Crowd Psychology and Ego Analysis, the founder of psychotherapy, Sigmund Freud, discusses mass formation and its ramifications, saying, “The strangest and at the same time most important phenomenon of mass formation is the increase in affectivity evoked in each individual (as) exaltation or intensification of emotion.”
The preeminent psychiatrist, Carl Jung, highlights mass formation in his prescient 1957 book, The Undiscovered Self, on the state of mankind and the dangers of modern materialism. His perspective is foundational, relative to Desmet’s recent findings:
“Under the influence of scientific assumptions, not only the psyche but the individual man and, indeed, all individual events whatsoever suffer a leveling down and a process of blurring that distorts the picture of reality into a conceptual average. We ought not to underestimate the psychological effect of the statistical world picture: it displaces the individual in favor of anonymous units that pile up into mass formations.”
Despite a wealth of historical precedents, the reaction to Desmet’s ideas was bizarre and unfounded. A renowned and respected psychotherapist had postulated that we might need to reconsider the unconscious response to lockdowns and mandates — and his ideas were summarily dismissed by the voice of the state.
The diagnosis is clear. Deriding mass formation and dismissing its influence during a global crisis is in itself a verification of the phenomenon. Mainstream media demonstrates how it perpetuates mass formation by indulging in another well-accepted psychological phenomenon: denial. Considering the degree of unwillingness to confront the reality of ineffectiveness and dangers of the COVID-19 vaccines, an evaluation of the news media’s response to the current plague can also be deemed delusional.
The Syndrome Persists
In recent decades, studies have shown that psychological problems are increasing geometrically. Rather than attempting to reverse this dysfunction, powerful forces in government and the corporate press continue to mislead and prey on an expanding susceptible population, who in the face of crisis, cling to authority.
It is the vulnerability of dissatisfied populations that allows mass formation.
Desmet suggests that a number of factors, including; isolation, a sense that life is meaningless — and particularly free-floating anxiety, frustration and aggression — independently or in unison, can lead to mass formation and its repercussions.
Jung also viewed precursors to dysfunction in the context of a modern age where the “State” and “Scientific Rationalism” play critical roles in supporting mass formation, saying:
“Science supplies us with, instead of the concrete individual, the names of organizations and, at the highest point, the abstract idea of the State as the principle of political reality. Apart from agglomerations of huge masses of people, in which the individual disappears anyway, one of the chief factors responsible for psychological mass-mindedness is scientific rationalism, which robs the individual of his foundations and his dignity. As a social unit he has lost his individuality and become a mere abstract number in the bureau of statistics. He can only play the role of an interchangeable unit of infinitesimal importance.”
The concept of mass formation and its relevance to the pandemic are undeniable when our current crisis is examined carefully, particularly when the inadequacies and inconsistencies of prevention and treatment are analyzed and understood.
Vaccines were initially presented as the only viable way to stem a deadly disease. A subsequent admission that they did not stop transmission was revealed in the context that they continued to be effective and safe. Any serious analysis of these claims confirms this also is a fabrication.
There is an important and viable inquiry asking how a false and deadly narrative continues to be accepted. Policies supporting repressive controls and ongoing vaccination have no foundation other than nonsensical dictates and support from a public bolstered with questionable data, prodded to near-hysteria.
The very forces that are responsible for the false narrative can only take a defensive position when light is shed on their methodology. The dogmatic negation of the idea that a mass formation is responsible for blind compliance and irrational acceptance of dangerous therapies is striking and revelatory.
As time passes, the induced fear and coerced consent will continue to be exposed as part of a scheme promoting selfish interests, and verifiably nothing to do with good health.
Eventually this epoch will be recognized for its essential impetus; the nefarious entrancement of a vulnerable world.
[...]
rwmalonemd.substack.com [2022-05-10] Robert W Malone MD, MS, David Marks, May 10, 2022 link archive General
Mattias Desmet, Professor of Clinical Psychology and author of the newly released, The Psychology of Totalitarianism, joins Del for an enthralling look at Mass Formation Psychology, the conditions that create, the threat it poses to society, and the key to breaking it.
thehighwire.com [2022-06-21] The HIGHWIRE, June 17, 2022 link archive General
Do you have faith in your doctor? Does he or she have your best interest in mind when they make decisions about your health? Maybe they do.
However, since Covid-CCP we are seeing that many doctors are being coerced into acting as puppets for hospital corporations and Big Pharma.
Defending The Republic has produced a documentary, Doctors Orders, on Covid-CCP issues. We have talked to honest, ethical doctors, scientists, patients and pharmacists who have gone back with us to the beginning of Covid hysteria.
They explain, with personal stories, how our medical system has failed us and continues to fail us - not to mention the failure of almost all media and the government.
This documentary is eye-opening. It's encouraging. It's hopeful.
There are simple, proven and inexpensive cures for Covid-CCP. It is immensely treatable. But the truth is: It is up to you to understand the science and advocate for yourself and your loved ones. You can NOT depend on your doctors to help you. You will learn in this documentary the real science and how to protect your health. Many of our freedoms in America depend on you studying this information and acting on it.
Ultimately, we must educate ourselves and take responsibility for doing all we can to stay healthy, take vitamins, exercise, stay informed, and stand up for our rights.
We at DefendingTheRepublic.org will do all we can to help you.
We ask that you watch so that you know the truth. And, as always, share the documentary with your family and friends.
rumble.com [2022-01-06] DefendingTheRepublic.org channel, December 10, 2021 link archive General
Stand for Health Freedom recently had the honor of sitting down with Holocaust survivor Vera Sharav and capturing her personal story on film. It’s a story that every individual needs to hear. A renowned champion of human rights and expert in biomedical research ethics, Ms. Sharav offers rare and valuable insights into the public health arena and state of emergency affecting each and every one of our lives. She also draws parallels between what happened in Nazi Germany and what’s happening in our society today — and discusses why it’s more important than ever for us to take a stand.
Mayer’s book [Milton Mayer, They Thought They Were Free] is frighteningly prescient; reading his words is like staring into our own souls. The following paragraphs will show just how similar the world’s response to covid has been to the German response to the “threat” of the Jews. If we can truly understand the parallels between our response to covid and the situation in Hitler’s Germany, if we can see what lies at the end of “two weeks to flatten the curve,” perhaps we can prevent the greatest atrocities from being fully realized in our own day. But to stop our bent toward tyranny, we must first be willing to grapple with the darkest parts of our nature, including our tendency to dehumanize others and to treat our neighbors as enemies.
Overcoming Decency
“Ordinary people—and ordinary Germans—cannot be expected to tolerate activities which outrage the ordinary sense of ordinary decency unless the victims are, in advance, successfully stigmatized as enemies of the people, of the nation, the race, the religion. Or, if they are not enemies (that comes later), they must be an element within the community somehow extrinsic to the common bond, a decompositive ferment (be it only by the way they part their hair or tie their necktie) in the uniformity which is everywhere the condition of common quiet. The Germans’ innocuous acceptance and practice of social anti-Semitism before Hitlerism had undermined the resistance of their ordinary decency to the stigmatization and persecution to come” (55).
Others have explained the link between totalitarian impulses and “institutionalized dehumanization” and have discussed the “othering” of unvaccinated persons in nations across the world. Mayer shows that such dehumanization does not necessarily begin with prejudice:
“National Socialism was anti-Semitism. Apart from anti-Semitism, its character was that of a thousand tyrannies before it, with modern conveniences. Traditional anti-Semitism . . . played an important role in softening the Germans as a whole to Nazi doctrine, but it was separation, not prejudice as such, that made Nazism possible, the mere separation of Jews and non-Jews” (116-117).
Even if many Germans did not harbor anti-Semitic prejudices (at least not initially), the forced separation of Jews and non-Jews created a devastating rift in German society, tearing the social fabric and paving the way for tyranny. In our day, the separation of the masked and unmasked, the vaccinated and the unvaccinated, has divided populations around the world like nothing we’ve experienced in our lifetimes. And the global scale of this separation has perhaps not happened in recorded history.
How has this separation been made possible? The immense power of propaganda, and particularly propaganda in the digital age. We think we understand how propaganda affects us, but we often don’t realize the truly insidious effects on how we view others until it is too late. Mayer’s friends explained this in great depth. On one occasion, Mayer asked the former bank clerk about one of his Jewish friends. “Did your memory of the peddler make you anti-Semitic?” “No—not until I heard anti-Semitic propaganda. Jews were supposed to do terrible things that the peddler had never done. . . . The propaganda didn’t make me think of him as I knew him but of him as a Jew” (124; emphasis added).
Is there anything we can do to mitigate the dehumanizing effects of propaganda? Mayer describes the power of Nazi propaganda as so intense that all of his friends were affected by it—changed by it—including the teacher who was more aware of such tactics. Nearly seven years after the war, his friends still could not be persuaded that they had been deceived:
“Nobody has proved to my friends that the Nazis were wrong about the Jews. Nobody can. The truth or falsity of what the Nazis said, and of what my extremist friends believed, was immaterial, marvelously so. There simply was no way to reach it, no way, at least, that employed the procedures of logic and evidence” (142).
Mayer’s conclusion is depressing. If we cannot persuade others with logic and evidence, how can we persuade them? How many of us have shared indisputable data that the vaccines carry risks? How many of us have shown videos where public health officials openly admit that the vaccines do not stop transmission and that cloth masks don’t work (and are in fact little more than “facial decorations”)? Yet the evidence does not persuade those who have been captured by propaganda; indeed, it cannot persuade them. This is because the very nature of propaganda does not appeal to logic or reason; it does not appeal to evidence. Propaganda appeals to our emotions, and in a world where many people are led by emotions, propaganda becomes deeply rooted in the hearts of those who consume it.
[...]
More information on Milton Mayer
brownstone.org [2022-08-10] JOSHUA STYLES, JULY 28, 2022 link archive General
Since the end of the Cold War, the concept of "globalization" has been one of the main topics of social sciences. Globalization is a controversial topic due to its main features and effects. Debates in this contex generally focuses on the "advantages and disadvantages" of globalization. On one side of these debates, some advocate that with globalization, people's lives have significantly improved and countries have started to develop rapidly, while, on the other side, some argue that nature, culture, and human life have faced grave threats and "global risk society" is being built. Debates on global risk society seem to have accelerated in recent years. With the COVID-19 outbreak, that emerged in China in December 2019 and went global, leading to a pandemic, it is seen that debates on "global risk society" started again in the media and among social scientists. This article aims to explore the effect of globalization on the spread of fear across the world by focusing on the case of COVID-19. Along with the basic characteristics of globalization, such as "widening," "deepening," and "acceleration," fear seems to have spread all over the world and have forced people to discuss the benefits and harms of globalization once more.
pubmed.ncbi.nlm.nih.gov [2022-02-06] Fatih Fuat Tuncer, July 13, 2020 link archive General
Pay close attention to the language used by both Prof Reicher and the language the newspaper article. The Professor’s words are ‘COVID surges. That’s why infection is spiking globally, lockdowns reimposed’. The newspaper refers to ‘Covid pandemic still growing exponentially’.
[...]
Is it possible that we are still anchored in ‘the fear’ of people falling down in the streets like those early videos from Wuhan? Has anyone seen that particular ‘symptom’ of the disease anywhere else in the world since then? https://twitter.com/Swift__Girl/status/1380604578501120006
[...]
Please take some time to reflect. Look at the statements of those in positions of power? Do they appear to be overestimating risks? Are they over-confident, certain that their measures are the right ones and that they will protect us? If this hypothesis is unsound, please tear it down with science. That is how science is supposed to work, after all.
bringbacknormal.ie [2021-05-14] 20 Apr, 2021 link archive General
My conjecture is that ‘perception of an enemy’ could be a Jungian archetype or a category of perception that represents a certain dynamic between groups of humans in societies or between humans and aspects of the world.
Humans are on one level tribal and it could be that tribal creatures have benefitted from being able to unify against a collective perception of an enemy, whether that be a pack of lions, another tribe or an individual within the tribe that must be exterminated or resolved at all costs for the tribe’s survival.
[...]
The devil, evil in general, witches, radical muslim terrorists, Jews, communists and coronavirus are all examples of phenomenon that have become, in some groups of peoples’ eyes, in some time in history, an unseen enemy.
Cases in point:
Witches: The Salem witch trials where any person could be a witch and therefore everyone had to be alert to the ‘unseen enemy.’
The data out of South Africa, after five weeks of Omicron spread, suggest that Omicron should be a cause for celebration, not fear. Its symptoms are mild to non-existent in the majority of the infected, especially the vaccinated; hospitalization rates are over nine times lower than for previous Covid strains; deaths are negligible. That assessment will only be confirmed as the US and other western countries gather their own data on Omicron.
Yet the public health establishment and the media are working overtime to gin up Omicron hysteria. The official response to the Omicron variant provides a case study in the deliberate manufacture of fear. The following strategies are key:
1. Create a group norm of fear
[...]
2. Buttress group fear with expert opinion
The only public health experts whom the media quote are those determined to put the most dire spin on Omicron. They stress worst-case hypothetical scenarios and dismiss actual good-case evidence. At best, they may grudgingly admit that Omicron symptoms are disproportionately mild, but rush to assert that there are still many as-yet unrealized grounds for worry. “Even if Omicron causes less severe cases, the sheer number of cases could once again overwhelm unprepared health systems,” the director-general of the World Health Organization said. “I’m not counting [Omicron’s lack of severity] as good news just yet,” a disease ecologist at Georgetown University said. “Even if infection is mild in many individuals, it’s not going to be mild in everyone.”
But that 100 percent mildness standard is unrealistic. There are outliers in any disease and any treatment; the question is: what is the predominant reality? The zero-risk, zero-harm standard for public policy adopted for the first time with Covid has proven a social, economic and public health disaster.
At worst, the favored experts do not even pay lip service to the evidence militating against panic. An epidemiologist at the University of North Carolina at Chapel Hill told the New York Times: “I think we need to be prepared for the possibility that this could be at least as bad as any previous wave that we’ve seen.” There are apparently no circumstances which would warrant a less-than-totalitarian response in advance of any actual disaster. The yearning for more draconian lockdowns and more control over the private sector is palpable.
3. Manufacture epistemological uncertainty and insist on that uncertainty as long as possible
[...]
4. Bury both good news and dissenters from the bad news
[...]
5. Omit relevant context
[...]
6. Flog the case count
[...]
spectatorworld.com [2022-01-03] Heather Mac Donald, December 20, 2021 link archive General
As José Ortega y Gasset makes clear in his masterful short essay “Heart and Head” no human being can ever do this.
“In any landscape, in any precinct where we open our eyes, the number of visible things is practically infinite, but in any given moment we can only see a very small number of them. The line of sight must fixate upon a small group of objects and deviate from the rest, effectively neglecting those other things. In other words, we cannot see one thing without ceasing to see others, without temporarily blinding ourselves to them. To see this thing means unseeing that one, in the same way that hearing one sound means unhearing others…. To see it is not enough that there exist, on one side, our organs of sight, and the other, the visible object situated, as always, between other equally visible things. Rather we must lead the pupil toward this object while withholding it from the others. To see, in short, it is necessary to focus. But to focus is precisely to seek something before seeing it, it is a sort of pre-see before the see. It thus seems that every vision supposes the existence of a pre-vision, which is not the product of either the pupil or the object, but rather another, pre-existing faculty charged with directing the eyes and exploring the surroundings, a thing called attention.”
In other words, human perceptions in a given moment are always mediated by previous and often quite personal cognitive, vital and sensorial experiences, and as a result, can never begin to approach the levels of neutrality or breadth of focus that we humans are presumed to be capable of having as participants in the empiricist paradigm of modernity.
Ortega thus suggests that we should—while never abandoning the search for enveloping truths—always retain a consciousness of the fact that many if not most descriptions proffered to us as exemplars of reality writ large are symbolic placeholders, or proxies, for the integral reality of the phenomenon in question.
[...]
Because they know most people—thanks in large part to the grave deficiencies of our educational system—have never been forced to ponder the problem of perception and how quite powerful forces are constantly creating and organizing mental structures, or epistemologies, designed to mediate between us and the vastness of reality, mediations designed to direct our attentions toward perceptions and interpretations that are invariably amenable to the interests of those very same powerful entities.
Indeed, one of the more common of these elite-imposed “suggestions” is precisely the idea that there is no one or any group of people imposing frames of interpretation upon the common people; that is, that we are always and everywhere addressing ourselves to the world with a virgin gaze.
Like large revenue-producing college athletic programs, Big Pharma is deeply aware of how little thought most citizens, and sadly it seems, most medical professionals give to how “facts” and notions of “reality” enter into their field of consciousness. And they play mercilessly upon this widespread epistemological illiteracy.
Take the PCR test.
Since the dawn of western medicine, medical diagnostics has been driven by symptomatology; that is, by having a physician cast his experienced eyes upon the physical manifestations of sickness in the patient. No symptoms, no diagnosis. No diagnosis, no treatment.
But what if you are the owner of a business that sells treatments and wants to expand its market share? Or a government leader, who might want to sow panic and division in a population so as to better control them?
Might it not be in each of their interests to generate a proxy of illness, one that would greatly inflate the numbers of those considered “sick” or “dangerous” and sell it to the population as being as grave and important as the real thing?
This is exactly what was done with the known-to-be-wildly-inaccurate-toward generating-false-positives PCR tests.
[...]
brownstone.org [2022-08-01] THOMAS HARRINGTON, AUGUST 1, 2022 link archive General
Why are media dialling back on the Covid hysteria? Is it because the “pandemic” is really over? Or is it an important part of the gaslighting process?
[...]
In another interview, with Fox News, Dr Walenksy said the CDC was going to publish data on how many people had died of Covid, and how many died with it.
This begs a series of important questions.
Why is the director of the CDC (seemingly) engaging with these Covid skeptic arguments after two years of pretending they don’t exist?
Why would Sky News air, and then tweet out, the video clip of a doctor challenging the health secretary?
In an unprecedented time, opportunities to thrive belong to those who embrace and adapt to the new normal of business. Learn about a new way to think about and manage work with Microsoft 365. Learn how Microsoft 365 and Microsoft Teams make it easier than ever for your team to organize, share and track files, lists, and tasks all in one place – so you save time and accomplish more together.
youtube.com [2022-03-10] Microsoft 365 channel, January 28, 2021 link archive General
Politicians and governments are suppressing science. They do so in the public interest, they say, to accelerate availability of diagnostics and treatments. They do so to support innovation, to bring products to market at unprecedented speed. Both of these reasons are partly plausible; the greatest deceptions are founded in a grain of truth. But the underlying behaviour is troubling.
Science is being suppressed for political and financial gain. Covid-19 has unleashed state corruption on a grand scale, and it is harmful to public health.1 Politicians and industry are responsible for this opportunistic embezzlement. So too are scientists and health experts. The pandemic has revealed how the medical-political complex can be manipulated in an emergency—a time when it is even more important to safeguard science.
bmj.com [2021-03-12] (pdf doc) Kamran Abbasi, The BMJ, London, UK, 13 November 2020 link archive General
I’m still trying to wrap my brain around the astonishing shift from the CDC on Tuesday, July 27, 2021. It is not just that the CDC is re-recommending masks for people indoors in many parts of the country, which could include your neighborhood or not, and this could change tomorrow. (Hint: right now, it disportionately affects red states.)
Whether and to what extent you “protect” yourself from disease with a paper strapped to your mouth and nose is now wholly contingent on data reporting and interpretation. It might feel like science but it has a better name: arbitrary power. Out with the Constitution. Out of traditions of law. Out with legislatures and the will of the people.
What’s even stranger was the rationale that the CDC cited to claim that the Delta variant renders the vaccines – the ones that have been hyped with unrelenting propaganda for many months, including stigmatization and demonization of those who refuse – substantially less effective for stopping infection than President Biden was touting just last week.
[...]
realclearmarkets.com [2021-07-30] By Jeffrey Tucker, July 30, 2021 link archive General
The COVID-19 pandemic is one of the most manipulated infectious disease events in history, characterized by official lies in an unending stream lead by government bureaucracies, medical associations, medical boards, the media, and international agencies.[3,6,57] We have witnessed a long list of unprecedented intrusions into medical practice, including attacks on medical experts, destruction of medical careers among doctors refusing to participate in killing their patients and a massive regimentation of health care, led by non-qualified individuals with enormous wealth, power and influence.
For the first time in American history a president, governors, mayors, hospital administrators and federal bureaucrats are determining medical treatments based not on accurate scientifically based or even experience based information, but rather to force the acceptance of special forms of care and “prevention”—including remdesivir, use of respirators and ultimately a series of essentially untested messenger RNA vaccines. For the first time in history medical treatment, protocols are not being formulated based on the experience of the physicians treating the largest number of patients successfully, but rather individuals and bureaucracies that have never treated a single patient—including Anthony Fauci, Bill Gates, EcoHealth Alliance, the CDC, WHO, state public health officers and hospital administrators.[23,38]
The media (TV, newspapers, magazines, etc), medical societies, state medical boards and the owners of social media have appointed themselves to be the sole source of information concerning this so-called “pandemic”. Websites have been removed, highly credentialed and experienced clinical doctors and scientific experts in the field of infectious diseases have been demonized, careers have been destroyed and all dissenting information has been labeled “misinformation” and “dangerous lies”, even when sourced from top experts in the fields of virology, infectious diseases, pulmonary critical care, and epidemiology. These blackouts of truth occur even when this information is backed by extensive scientific citations from some of the most qualified medical specialists in the world.[23] Incredibly, even individuals, such as Dr. Michael Yeadon, a retired ex-Chief Scientist, and vice-president for the science division of Pfizer Pharmaceutical company in the UK, who charged the company with making an extremely dangerous vaccine, is ignored and demonized. Further, he, along with other highly qualified scientists have stated that no one should take this vaccine.
For example, much of what has happened throughout the COVID-19 pandemic parallels the early days of the AIDS epidemic. Fauci fought to keep a variety of effective treatments for AIDS off the market so that he could push through a deadly and ineffective (but highly lucrative) drug on the gay community to treat HIV, which was AZT. This is exactly what Fauci later did during COVID-19, first with remdesivir, and later the vaccines, except this time it affected all of America rather than just the gay community (who actively protested him at the time, but for all practical purposes were ignored):
Note: many trial participants were severely injured in the AZT trials. These events were of course covered up so AZT could be pushed on America.
Similarly, there were significant concerns with safety, efficacy, and research fraud, which should have never allowed the first selective serotonin reuptake inhibitor (SSRI) antidepressant (Prozac) to enter the market. Bush senior (who had previously served on the board of Prozac's manufacturer) played a crucial role in nonetheless forcing Prozac through the approval process.
Once it was approved (many other competitors quickly jumped into the market with equally dubious clinical trial data), the FDA received a deluge of reports of severe side effects from SSRI users, including violent acts of suicide or homicide. The FDA then did everything it could to bury this information (e.g., forbidding their reviewer to release a report that was critical of giving SSRIs to children and authoring its own inaccurate meta-analysis, which erroneously argued that there were no safety concerns with the SSRIs).
Eventually, after two decades of protest against the FDA, which included a congressional hearing, the agency capitulated by issuing a black box warning (used for medications known to carry serious safety risks) on the SSRIs, which has since been mostly ignored. As that represents the closest documented case precedent to what is happening now with the COVID-19 vaccines, I tried to document what the FDA did then here (it is also covered in more detail in this book).
Similarly, in 2009, in response to widespread publicity detailing severe adverse events attributed to the Human Papillomavirus (HPV) vaccine, the FDA and CDC initiated a study to examine Gardasil's safety profile based on VAERS case reports. It analyzed all VAERS reports filed since Gardasil's mid-2006 approval through the end of 2008, a period of two and a half years.
The study found that "the VAERS reporting rate for [Gardasil] is triple the rate for all other vaccines combined." Additionally, the study found that 68% of the reports were submitted by representatives of Merck, Gardasil's manufacturer, most of which needed to be completed or more accurate, and 90% of which required more information essential for conducting medical assessments. Finally, the authors also noted that VAERS suffered from underreporting.
Despite that red flag and a clear indication that, if anything, it was underestimating the scale of the issue, the authors just dismissed it. Instead, they declared that the high rate of adverse events "reflects greater public attention to HPV," which was purportedly "stimulated" by "widespread media coverage" and that Gardasil's "post-licensure safety profile" as calculated from VAERS data is "broadly consistent" with safety data collected in its clinical trials, while simultaneously failing to support these assertions. Not surprisingly, following the study's publication, news organizations and health authorities such as the CDC and WHO repeatedly referenced it as proof that Gardasil was safe.
Note: I consider the original smallpox vaccines, the anthrax vaccine, the HPV vaccine and the COVID-19 vaccines to be the most harmful vaccines that ever entered the market. For this reason, I have tried to illustrate many of the forgotten lessons with the others to provide the context to explain how the COVID-19 vaccines could have possibly been approved and then mandated rather than being withdrawn once countless red flags emerged.
Given how poorly the HPV vaccine was handled, I was dubious that the CDC or FDA could be relied upon to recognize red alerts within VAERS for a highly dangerous vaccine entering the market. However, VAERS providing red warnings (which were ignored) also demonstrates that VAERS is serving its intended function because its creation was the result of activists (e.g., parents of vaccine-injured children) demanding a way for the public to be able to directly report vaccine injuries and be able to access this citizen data as they had dealt with years of doctors and the government deliberately covering those injuries up.
This was necessary because medical providers and the government frequently placed insurmountable obstacles in the way of reporting vaccine injuries, and VAERS was a concession that was given in exchange for the vaccine manufacturers being absolved of all liability for vaccine injuries in the 1986 law. Since the CDC, by law, cannot censor VAERS (although, as recent events have shown, they still often do), the government and the media actively disparage the validity of VAERS (except when it can be cited to prove safety). Instead, VAERS requires the public to use the system to illuminate vaccine safety concerns that those in power would prefer to remain hidden.
All of this is best highlighted by what has occurred with the COVID-19 vaccines. In addition to numerous other red flags with the vaccines, VAERS has also demonstrated that the COVID-19 vaccines are by far the most dangerous vaccines in history, and many members of the public have been able to use VAERS to draw attention to this issue. However, like the previous contender for the most dangerous vaccine in history (Gardasil), those VAERS signals have been ridiculed by the media and ignored by our health authorities. The most conclusive proof of this is a recent FOIA which proved that the CDC has intentionally ignored hundreds of COVID-19 safety signals from VAERS.
[...]
amidwesterndoctor.substack.com [2023-07-17] A Midwestern Doctor, July 16, 2023 link archive General
We investigate why the USA, unlike Canada and Western European countries, has a sustained exceedingly large mortality in the “COVID-era” occurring from March 2020 to present (October 2021). All-cause mortality by time is the most reliable data for detecting true catastrophic events causing death, and for gauging the population-level impact of any surge in deaths from any cause. The behaviour of the USA all-cause mortality by time (week, year), by age group, by sex, and by state is contrary to pandemic behaviour caused by a new respiratory disease virus for which there is no prior natural immunity in the population. Its seasonal structure (summer maxima), age-group distribution (young residents), and large state-wise heterogeneity are unprecedented and are opposite to viral respiratory disease behaviour, pandemic or not. We conclude that a pandemic did not occur. We infer that persistent chronic psychological stress induced by the long-lasting government-imposed societal and economic transformations during the COVID-era converted the existing societal (poverty), public-health (obesity) and hot-climate risk factors into deadly agents, largely acting together, with devastating population-level consequences against large pools of vulnerable and disadvantaged residents of the USA, far above preexisting pre-COVID-era mortality in those pools. We also find a large COVID-era USA pneumonia epidemic that is not mentioned in the media or significantly in the scientific literature, which was not adequately addressed. Many COVID-19-assigned deaths may be misdiagnosed bacterial pneumonia deaths. The massive vaccination campaign (380 M administered doses, 178 M fully vaccinated individuals, mainly January-August 2021 and March-August 2021, respectively) had no detectable mitigating effect, and may have contributed to making the younger population more vulnerable (35-64 years, summer-2021 mortality).
[Emphasis added]
See related data element: 2023-06-22 ::: There Was No Pandemic (essay)
researchgate.net [2021-12-15] Denis G Rancourt, Marine Baudin, Jérémie Mercier, October 2021 link archive General
I am an accomplished interdisciplinary scientist and physicist, and a former tenured Full Professor of physics and lead scientist, originally at the University of Ottawa.
I have written over 30 scientific reports relevant to COVID, starting April 18, 2020 for the Ontario Civil Liberties Association (ocla.ca/covid), and recently for a new non-profit corporation (correlation‑canada.org/research). Presently, all my work and interviews about COVID are documented on my website created to circumvent the barrage of censorship (denisrancourt.ca).
In addition to critical reviews of published science, the main data that my collaborators and I analyse is all‑cause mortality.
All-cause mortality by time (day, week, month, year, period), by jurisdiction (country, state, province, county), and by individual characteristics of the deceased (age, sex, race, living accomodations) is the most reliable data for detecting and epidemiologically characterizing events causing death, and for gauging the population-level impact of any surge or collapse in deaths from any cause.
Such data is not susceptible to reporting bias or to any bias in attributing causes of death. We have used it to detect and characterize seasonality, heat waves, earthquakes, economic collapses, wars, population aging, long-term societal development, and societal assaults such as those occurring in the COVID period, in many countries around the world, and over recent history, 1900-present.
Interestingly, none of the post-second-world-war Centers-for-Disease-Control-and-Prevention-promoted (CDC‑promoted) viral respiratory disease pandemics (1957-58, “H2N2”; 1968, “H3N2”; 2009, “H1N1 again”) can be detected in the all‑cause mortality of any country. Unlike all the other causes of death that are known to affect mortality, these so‑called pandemics did not cause any detectable increase in mortality, anywhere.
The large 1918 mortality event, which was recruited to be a textbook viral respiratory disease pandemic (“H1N1”), occurred prior to the inventions of antibiotics and the electron microscope, under horrific post-war public-sanitation and economic-stress conditions. The 1918 deaths have been proven by histopathology of preserved lung tissue to have been caused by bacterial pneumonia. This is shown in several independent and non-contested published studies.
My first report analysing all-cause mortality was published on June 2, 2020, at censorship-prone Research Gate, and was entitled “All-cause mortality during COVID-19 - No plague and a likely signature of mass homicide by government response”. It showed that hot spots of sudden surges in all‑cause mortality occurred only in specific locations in the Northern-hemisphere Western World, which were synchronous with the March 11, 2020 declaration of a pandemic. Such synchronicity is impossible within the presumed framework of a spreading viral respiratory disease, with or without airplanes, because the calculated time from seeding to mortality surge is highly dependent on local societal circumstances, by several months to years. I attributed the excess deaths to aggressive measures and hospital treatment protocols known to have been applied suddenly at that time in those localities.
The work was pursued in greater depth with collaborators for several years and continues. We have shown repeatedly that excess mortality most often refused to cross national borders and inter-state lines. The invisible virus targets the poor and disabled and carries a passport. It also never kills until governments impose socio-economic and care-structure transformations on vulnerable groups within the domestic population.
Here are my conclusions, from our detailed studies of all-cause mortality in the COVID period, in combination with socio-economic and vaccine-rollout data:
If there had been no pandemic propaganda or coercion, and governments and the medical establishment had simply gone on with business as usual, then there would not have been any excess mortality
There was no pandemic causing excess mortality
Measures caused excess mortality
COVID-19 vaccination caused excess mortality
Regarding the vaccines, we quantified many instances in which a rapid rollout of a dose in the imposed vaccine schedule was synchronous with an otherwise unexpected peak in all-cause mortality, at times in the seasonal cycle and of magnitudes that have not previously been seen in the historic record of mortality.
In this way, we showed that the vaccination campaign in India caused the deaths of 3.7 million fragile residents. In Western countries, we quantified the average all-ages rate of death to be 1 death for every 2000 injections, to increase exponentially with age (doubling every additional 5 years of age), and to be as large as 1 death for every 100 injections for those 80 years and older. We estimated that the vaccines had killed 13 million worldwide.
Many of us are independently coming to this conclusion .
My summary is thus:
that a virus, was circulating the globe in 2019/20, which may or may not have been the result of gain-of-function research, which nevertheless was not particularly novel and otherwise, if ignored, would not have made any material impact on mortality in any particular country;
that the response to news of this virus was responsible for the deaths of millions of people worldwide but only moribund people whose lives were curtailed by 6 to 12 months;
that those deaths were attributed to the virus due to inappropriate use of the PCR test on too high a cycle threshold;
that if any other virus, even say any of the 200 that comprise the “common cold” had been singularly tested in the same way, their presence in the deceased would have produced the same alleged deaths as COVID;
that the impact of these policy deaths would have been net off the following mortality year, due to the “pull-forward” effect except for the “vaccine” generating a new cohort of accelerated moribundity;
that these “vaccine” deaths were falsely attributed to COVID in the same way as the original pandemic;
that the excess mortality in the years post the original proclamation of a pandemic, and the introduction of the novel therapy to deal with it, appears lower than it really is because it includes the hidden deficit of those who died slightly prematurely the previous year;
that even with all that, the degree of life years lost (as opposed to absolute deaths) has never constituted an emergency, notwithstanding the much lower age profiles of deaths since the “vaccine”, compared to deaths before.
denisrancourt.ca [2023-06-29] Denis Rancourt, Jun 22, 2023 link archive General
Suddenly, Biden announces the pandemic is over as the narrative is now collapsing from all sides. From boosters to kids shots, the vaccine push is faltering as lawsuits pile up to remove the last covid restrictions.
These measures are being imposed in a country that, since 2012, has seen an exponential growth in child poverty to potentially sub-Victorian levels. In March 2019, the number of children living in "absolute poverty" grew by a staggering 200,000 in a twelve-month period, to a total of 3.7 million. How will this number be further impacted by lockdown?
How did we arrive at this point? Who steered the UK Government towards this questionable and alarmist lockdown policy? The unexamined assumption is that conclusions were formed on the basis of sound epidemiological analysis and research by doctors and scientists who care about our welfare.
The reality is what we will examine in this article. [...]
Various investigators conduct investigations, in collaboration with lawyers and advocates. The 2nd Nuremberg Tribunal is a fact. Its act has been in preparation for months now.
This is under the leadership of German lawyer Dr. Reiner Fuellmich, who is currently filing a class action. What is a class action? A class action, also called a representative action or group claim, is a form of jurisprudence in which a large group of people collectively bring a claim before the court or in which a certain class of defendants is prosecuted.
And now good news from Norway:
A group of researchers from Norway have filed a lawsuit against the corona policy.
The Norwegian government is being sued for crimes against humanity.
America’s Frontline Doctors filed a motion to stop the use of Emergency Use Authorization COVID vaccines for anyone under 18, anyone with natural immunity or anyone who hasn’t received informed consent.
More information on America’s Frontline Doctors
More information on the lawsuit: America's Frontline Doctors vs US Department of Health and Human Services (HHS)
childrenshealthdefense.org [2021-07-23] By Megan Redshaw, 07/20/21 link archive Lawsuits/Legal Counsel
In this exclusive interview, Spiro is joined by Attorney Ana Garner who is a member of the legal team that recently filed a lawsuit against the Secretary of the Department of Health and Human Services (HHS).
The lawsuit is focused on the experimental Covid vaccine, the Emergency Use Authorization (EUA) and includes sworn testimony from a whistleblower alleging the government reporting systems for adverse reactions to the Covid vaccine is under-reporting deaths by at least five times and projects the real numbers are closer to 45,000 people who died after receiving the vaccine.
British officials and the most influential figures in public health have been accused of genocide, citing a series of statistics on the impact of “vaccines” and policies introduced under the guise of “COVIDA mitigation”.
The group, including the former vice-president of Pfizer, dr. Michael Yeadon, has filed a lawsuit with the International Criminal Court (ICC) (worth reading) on behalf of British citizens against Boris Johnson and British officials, Bill and Melinda Gates, CEOs of major pharmaceutical companies and World Economic Forum CEO Klaus Schwab and others for crimes against humanity.
The ICC accepted the matter and assigned the following reference number OTP-CR-473/21.
Among the accused are:
Dr. Anthony Fauci;
Tedros Adhanom Ghebreyesus, Director-General of the World
Health Organization (WHO);
June Raine, Executive Director of the Medicines and Health
Products Regulatory Agency (MHRA);
Dr. Radiv Shah, President of the Rockefeller Foundation; and
Dr. Peter Daszak, President of the EcoHealth Alliance, as “responsible for a number of violations of the Nuremberg Code ... of war crimes and crimes of aggression” in the UK and other countries.
Albert Burla, CEO of Pfizer
Stephane Bancel, CEO of AstraZeneca
Pascal Soriot, CEO of Moderna
Alex Gorski, CEO of Johnson and Johnson
Boris Johnson, Prime Minister of the United Kingdom
Christopher Whitty, Chief Health Adviser in the UK
Matthew Hancock, Former British Secretary of State for Health and Welfare
Klaus Schwab, President of the World Economic Forum
After repeated unsuccessful attempts to bring the case before the English justice system, prosecutors demanded "urgent" to "stop the distribution of COVID vaccines, introduce illegal vaccination passports and all other types of illegal warfare" against UK residents.
The group's lawsuit, filed on December 6, claims that the "vaccines" against the experimental gene therapy COVID-19 were based on research into increased coronary activity of the bat virus, claiming that these "vaccines" caused mass deaths and injuries, and that the United Kingdom Government has failed to investigate such reported deaths and injuries.
that the number of COVID patients and deaths was artificially inflated; that masks are harmful due to hypoxia, hypercapnia and other consequences;
and PCR tests are "completely unreliable" and "contain carcinogenic ethylene oxide".
Forty-seven percent of very liberal adults said that they believed Covid presented a “great risk” to their own personal health and well-being. That was a significantly larger share than among conservatives, moderates or even liberals who stopped short of calling themselves very liberal. Particularly striking was the level of concern among liberals under age 45, even though the virus’s worst effects have been concentrated among older people.
I understand why attitudes about the virus vary so sharply by ideology. Our country is polarized on most high-profile issues today. In the case of Covid, Donald Trump and some other Republicans exacerbated the divide by making a series of false statements that downplayed the threat or misrepresented the vaccines.
To many liberals, taking Covid seriously — more seriously, at times, than the scientific evidence justified — became an expression of identity and solidarity. As one progressive activist tweeted last year, “The inconvenience of having to wear a mask is more than worth it to have people not think I’m a conservative.”
[...]
Rebuttal of poll data interpretations : Trends in COVID Anxiety, Robert Malone, August 31, 2022
nytimes.com [2022-09-01] David Leonhardt, Aug. 31, 2022 link archive General
While most of the public continue to have confidence in the benefits of childhood vaccines for measles, mumps, and rubella, the experience of the COVID-19 pandemic and debates over vaccine requirements and mandates appear to have had an impact on public attitudes towards MMR vaccine requirements for public schools. The latest KFF COVID-19 Vaccine Monitor survey finds that about seven in ten adults (71%) say healthy children should be required to get vaccinated for MMR in order to attend public schools, down from 82% who said the same in an October 2019 Pew Research Center poll. Almost three in ten (28%) now say that parents should be able to decide not to vaccinate their school-age children, even if this creates health risks for others, up from 16% in 2019. Among Republicans and Republican-leaning independents, there has been a 24 percentage-point increase in the share who hold this view (from 20% to 44%).
With COVID-19 cases rising across the country, just about a third of adults say they are worried they will get seriously sick from COVID-19, though nearly half of the public say they are worried about an increase in COVID-19 cases and hospitalizations in the U.S. this winter. As previous KFF surveys have repeatedly found, Black and Hispanic adults continue to be more concerned about the pandemic compared to White adults, with about two-thirds of Black adults (68%) and Hispanic adults (69%) saying they are worried about an increase in cases and hospitalizations this winter, compared to about four in ten White adults who say the same. Older adults are more likely than those under age 65 to say they are worried they will get seriously sick from COVID-19 (43% vs. 34%) and that cases and hospitalizations will rise this winter (60% vs. 46%).
As the country faces a “tripledemic”, with a surge in flu and RSV (respiratory syncytial virus) cases accompanying the rise in COVID-19 cases, many parents are now concerned about not one, but all three of these viruses. About half of parents are worried their child will get seriously sick from COVID-19 or the flu. A slight majority of parents (56%) say they are worried their child will get seriously sick from RSV – rising to more than seven in ten parents with a child under the age of 5 (73%), an age group that is particularly vulnerable to RSV.
Though many no longer see COVID-19 as a uniquely urgent threat, public health officials continue to encourage vaccination and emphasize the importance of the updated bivalent booster to help prevent serious illness and death from COVID-19, particularly in light of holiday gathering and travel. However, public uptake of the updated booster is relatively tepid, with just about one in five adults saying they have already gotten it. Democrats (38%) and adults ages 65 and older (39%) have been more eager, with about four in ten saying have already gotten the updated COVID-19 booster which has been available since September. Fewer young adults under the age of 30 (11%) and Republicans (12%) report having gotten an updated booster dose.
Though public health officials have stressed the importance of the updated COVID-19 booster for older adults who are more vulnerable to complications from a COVID infection, more than half of adults ages 65 and older have not yet gotten the updated booster. About a third (36%) of vaccinated adults ages 65 and older who have not yet gotten the bivalent booster say they don’t think they need it (36%) and a similar share say they don’t think the benefit of the updated booster is worth it.
Vaccinated Republicans and Republican-leaning independents are particularly skeptical of the value of the updated booster with about two-thirds of those who have not yet gotten it saying they don’t think they need it (64%) and that the benefit is not worth it (61%) while Democrats are most likely to say they have been too busy or haven’t had the time to get the update booster (51%).
[...]
kff.org [2022-12-20] Lunna Lopes, Shannon Schumacher, Grace Sparks, Marley Presiado, Liz Hamel, Mollyann Brodie, December 2022 link archive General
“33% of Democrats nationally believe that someone they know may have died from side effects of the COVID-19 vaccine.”
It seems the dam is truly breaking after all. A new Rasmussen poll – recently shared on Twitter – shows a staggering shift in what Democrats once believed to be true about the COVID-19 injections.
But before we look at the latest data, let’s recap another Rasmussen poll from December 2021 — and then compare that to the one just released.
Democrats were the most highly vaccinated and most likely to dismiss natural immunity.
[...]
December 15-16, 2021, Democrats had a significantly higher vaccination rate than Republicans: 60% (R) vs. 80% (D), a 20% difference.
[...]
Now fast-forward to January 9, 2023.
The apparent turnaround is astonishing. “51% of Democrats nationally believe it is likely the vaccines have caused a significant number of unexplained deaths, 40% of Democrats do not.”
[...]
dailyclout.io [2023-01-12] The Vigilant Fox, January 11, 2023 link archive General
Nearly a quarter of Americans believe someone they know died from COVID-19 vaccine side effects, and even more say they might be willing to become plaintiffs in a class-action lawsuit against vaccine makers.
The latest Rasmussen Reports national telephone and online survey finds that 24% of American Adults say they know someone personally who died from side effects of the COVID-19 vaccine. Sixty-nine percent (69%) don’t know anyone who died from being vaccinated against the virus. (To see survey question wording, click here.)
Forty-two percent (42%) say that, if there was a major class-action lawsuit against pharmaceutical companies for vaccine side effects, they would be likely to join the lawsuit, including 24% who say it’s Very Likely they’d join such a lawsuit. Forty-seven percent (47%) aren’t likely to join a class-action lawsuit against vaccine makers, including 25% who say it’s Not At All Likely. Another 11% are not sure.
The survey of 1,110 American Adults was conducted on October 26 and 29-30, 2023 by Rasmussen Reports. The margin of sampling error is +/- 3 percentage points with a 95% level of confidence. Field work for all Rasmussen Reports surveys is conducted by Pulse Opinion Research, LLC. See methodology.
Nearly half (47%) say they know someone personally who died from the COVID-19 virus, while 49% don’t know anyone who died from the virus, which became a pandemic in the United States in 2020.
Their latest survey, released at 10:30am EST on November 2, confirms (yet again) that the COVID vaccine is a train wreck, the biggest healthcare disaster in our lifetime.
The key conclusions:
47% personally know someone who was killed by the COVID virus
24% personally know someone who was killed by the COVID vaccine.
42% said it was somewhat likely or very likely they would join a major class-action lawsuit against pharmaceutical companies for vaccine side effects. That would make it the largest class action in US history by a long shot.
The implications are stunning:
56% of people who got vaccinated are or were vaccine injured in some way. This is because 42% want to sue but only 75% were vaccinated. So 42/75=56%. That is is unprecedented; a complete train wreck for a vaccine that was touted as “safe and effective.”
If you believe 1M people died from COVID, then this poll suggests that 500K people died from the COVID vaccine (computed as 24/47×1.1M killed from COVID virus using the two numbers above from the survey).
When the 911 terrorist attacks killed almost 3,000 people, it was major news. When the US government kills 500,000 Americans, there are no headlines and no investigations. This is the biggest story in America today.
Bottom line: Heads should roll. Now. Let the finger-pointing begin!
The controversy over whether the SARS-CoV-2 virus has ever been isolated or purified continues. However, using the above definition, common sense, the laws of logic and the dictates of science, any unbiased person must come to the conclusion that the SARS-CoV-2 virus has never been isolated or purified. As a result, no confirmation of the virus’ existence can be found. The logical, common sense, and scientific consequences of this fact are:
the structure and composition of something not shown to exist can’t be known, including the presence, structure, and function of any hypothetical spike or other proteins;
the genetic sequence of something that has never been found can’t be known;
“variants” of something that hasn’t been shown to exist can’t be known;
it’s impossible to demonstrate that SARS-CoV-2 causes a disease called Covid-19.
andrewkaufmanmd.com [2021-07-02] Dr. Andrew Kaufman, MD, Dr. Thomas Cowan, MD, Sally Fallon Morell, MA, February 18, 2021 link archive General
Around the world, people are sequencing and sharing SARS-CoV-2 genomic data. The Nextstrain team analyzes these data on a global and continental level. More specific analysis are often performed by groups around the world. This page lists publicly available SARS-CoV-2 analyses that use Nextstrain from groups all over the world. In addition to exploring SARS-CoV-2 evolution in finished analyses, you can use our new Nextclade tool to compare your sequences to the SARS-CoV-2 reference sequence, assign them to clades, and see where they fall on a the SARS-CoV-2 tree.
This is in response to your request made under the Access to Information Act (the Act) for the following information:
All records describing the isolation of a SARS-COV-2 virus, directly from a sample taken from a diseased patient, where the patient sample was not first combined with any other source of genetic material (i.e. monkey kidney cells aka vero cells; liver cancer cells).
[...]
Having completed a thorough search, we regret to inform you that we were unable to locate any records responsive to your request.
[...]
[See collection of more responses from Christine Massey's FOI requests on the isolated virus.]
More information on Christine Massey
fluoridefreepeel.ca [2021-08-05] (pdf doc) June 13, 2020 link archive General
The emergence of COVID-19 disease due to SARS-CoV-2 at the end of 2019 was rapidly associated with the isolation of the strain from co-culture onto VERO cells. These isolations quickly made it possible to carry out the first tests for antiviral agents’ susceptibility and drug repurposing. However, it seems important to make an inventory of all the cells that can support the growth of this virus and evaluate possible differences between isolates. In the present work, we tested 4 strains of SARS-CoV-2 locally isolated on a panel of 34 cell lines present in our laboratory and commonly used for the isolation of human pathogenic microorganism. After inoculation, cells were observed for cytopathic effects and quantitative real-time polymerase reaction was used to measure the virus replication on the cells. We were able to obtain growth on 7 cell lines, 6 simian, and the human Caco-2. The cytopathogenic effects are variable, ranging from lysis of the cell monolayer in 48–72 h to no cytopathic effect in spite of intense multiplication, as in Caco-2 cells. Interestingly, effect and multiplication varied widely according to the strain tested. In this paper, we explored the species specificity and tissue tropism of SARS-CoV-2 in vitro on a panel of cells available in our laboratory and identified human and animal cell lines susceptible to support SARS-CoV-2 replication. Our work highlights the importance of testing multiple strains when testing antiviral molecules and performing patho-physiological analyzes.
ncbi.nlm.nih.gov [2022-10-09] Nathalie Wurtz, Gwilherm Penant, ..., Bernard La Scola, Jan 2, 2021 link archive General
Immunocompromised adults can have prolonged acute respiratory syndrome coronavirus 2 (SARS-CoV-2) positive RT-PCR results, long after the initial diagnosis of coronavirus disease 2019 (COVID-19). This study aimed to determine if SARS-CoV-2 virus can be recovered in viral cell culture from immunocompromised adults with persistently positive SARS-CoV-2 RT-PCR tests. We obtained 20 remnant SARS-CoV-2 PCR positive nasopharyngeal swabs from 20 immunocompromised adults with a positive RT-PCR test ≥14 days after the initial positive test. The patients' 2nd test samples underwent SARS-CoV-2 antigen testing, and culture with Vero-hACE2-TMPRSS2 cells. Viral RNA and cultivable virus were recovered from the cultured cells after qRT-PCR and plaque assays. Of 20 patients, 10 (50%) had a solid organ transplant and 5 (25%) had a hematologic malignancy. For most patients, RT-PCR Ct values increased over time. There were 2 patients with positive viral cell cultures; one patient had chronic lymphocytic leukemia treated with venetoclax and obinutuzumab who had a low viral titer of 27 PFU/mL. The second patient had marginal zone lymphoma treated with bendamustine and rituximab who had a high viral titer of 2 x 106 PFU/mL. Most samples collected ≥7 days after an initial positive SARS-CoV-2 RT-PCR had negative viral cell cultures. The 2 patients with positive viral cell cultures had hematologic malignancies treated with chemotherapy and B cell depleting therapy. One patient had a high concentration titer of cultivable virus. Further data are needed to determine risk factors for persistent viral shedding and methods to prevent SARS-CoV-2 transmission from immunocompromised hosts.
pubmed.ncbi.nlm.nih.gov [2022-10-09] Abby Sung, Adam L Bailey, .., Jennie H Kwon, Feb 2, 2022 link archive General
Severe acute respiratory syndrome coronavirus 2 viral load in the upper respiratory tract peaks around symptom onset and infectious virus persists for 10 days in mild-to-moderate coronavirus disease (n = 324 samples analysed). RT-PCR cycle threshold (Ct) values correlate strongly with cultivable virus. Probability of culturing virus declines to 8% in samples with Ct > 35 and to 6% 10 days after onset; it is similar in asymptomatic and symptomatic persons. Asymptomatic persons represent a source of transmissible virus.
pubmed.ncbi.nlm.nih.gov [2022-10-09] Anika Singanayagam, Monika Patel, ..., Robin Gopal, August 2020 link archive General
Coronavirus disease 2019 (COVID-19), which is caused by infection with the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has become a global pandemic. It is unclear whether convalescing patients have a risk of reinfection. We generated a rhesus macaque model of SARS-CoV-2 infection that was characterized by interstitial pneumonia and systemic viral dissemination mainly in the respiratory and gastrointestinal tracts. Rhesus macaques reinfected with the identical SARS-CoV-2 strain during the early recovery phase of the initial SARS-CoV-2 infection did not show detectable viral dissemination, clinical manifestations of viral disease, or histopathological changes. Comparing the humoral and cellular immunity between primary infection and rechallenge revealed notably enhanced neutralizing antibody and immune responses. Our results suggest that primary SARS-CoV-2 exposure protects against subsequent reinfection in rhesus macaques.
science.org [2022-10-09] WEI DENG, LINLIN BAO, ..., CHUAN QIN, 2 Jul 2020 link archive General
We recently reported the development of the first African green monkey (AGM) model for COVID-19 based on a combined liquid intranasal (i.n.) and intratracheal (i.t.) exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Here, we followed up on this work by assessing an i.n. particle only route of exposure using the LMA mucosal atomization device (MAD). Six AGMs were infected with SARS-CoV-2; three animals were euthanized near the peak stage of virus replication (day 5) and three animals were euthanized during the early convalescence period (day 34). All six AGMs supported robust SARS-CoV-2 replication and developed respiratory disease. Evidence of coagulation dysfunction as noted by a transient increases in aPTT and circulating levels of fibrinogen was observed in all AGMs. The level of SARS-CoV-2 replication and lung pathology was not quite as pronounced as previously reported with AGMs exposed by the combined i.n. and i.t. routes; however, SARS-CoV-2 RNA was detected in nasal swabs of some animals as late as day 15 and rectal swabs as late as day 28 after virus challenge. Of particular importance to this study, all three AGMs that were followed until the early convalescence stage of COVID-19 showed substantial lung pathology at necropsy as evidenced by multifocal chronic interstitial pneumonia and increased collagen deposition in alveolar walls despite the absence of detectable SARS-CoV-2 in any of the lungs of these animals. These findings are consistent with human COVID-19 further demonstrating that the AGM faithfully reproduces the human condition.
virologyj.biomedcentral.com [2022-10-09] Robert W. Cross, Krystle N. Agans, ..., Thomas W. Geisbert, 18 August 2020 link archive General
SARS-CoV-2 is an emerging pathogen that has already had catastrophic consequences on the health and well-being of people worldwide. As a zoonotic virus, the implications for animal populations are largely unknown. This manuscript describes a pilot study in which domestic cats and dogs were assessed for their susceptibility to infection. While neither species developed clinical disease in this study, cats shed infectious virus for up to 5 d and infected naive cats via direct contact, while dogs do not appear to shed virus. Cats that were reinfected with SARS-CoV-2 mounted an effective immune response and did not become reinfected. These studies have important implications for animal health and suggest that cats may be a good model for vaccine development.
Abstract
The pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has reached nearly every country in the world with extraordinary person-to-person transmission. The most likely original source of the virus was spillover from an animal reservoir and subsequent adaptation to humans sometime during the winter of 2019 in Wuhan Province, China. Because of its genetic similarity to SARS-CoV-1, it is probable that this novel virus has a similar host range and receptor specificity. Due to concern for human–pet transmission, we investigated the susceptibility of domestic cats and dogs to infection and potential for infected cats to transmit to naive cats. We report that cats are highly susceptible to infection, with a prolonged period of oral and nasal viral shedding that is not accompanied by clinical signs, and are capable of direct contact transmission to other cats. These studies confirm that cats are susceptible to productive SARS-CoV-2 infection, but are unlikely to develop clinical disease. Further, we document that cats developed a robust neutralizing antibody response that prevented reinfection following a second viral challenge. Conversely, we found that dogs do not shed virus following infection but do seroconvert and mount an antiviral neutralizing antibody response. There is currently no evidence that cats or dogs play a significant role in human infection; however, reverse zoonosis is possible if infected owners expose their domestic pets to the virus during acute infection. Resistance to reinfection holds promise that a vaccine strategy may protect cats and, by extension, humans.
pnas.org [2022-10-09] Angela M. Bosco-Lauth, Airn E. Hartwig, ..., Richard A. Bowen, September 29, 2020 link archive General
From infectious disease and computer malware to the rapid success of online marketing campaigns
With the coronavirus epidemic sparking a global health scare, it can be hard to keep up with the terminological developments.
For the official name of the disease caused by the virus, the World Health Organization has settled on “Covid-19,” short for “coronavirus disease 2019.” While the outbreak is thought to have emerged from an animal and seafood market in Wuhan, China, health officials have avoided naming the disease after its place of origin. “Having a name matters to prevent the use of other names that can be inaccurate or stigmatizing,” WHO chief Tedros Adhanom Ghebreyesus told reporters earlier this month—although that hasn’t stopped people from giving the disease names like “Wuhan flu” or even “Wuflu.”
[...]
wsj.com [2022-04-14] By Ben Zimmer, Feb. 21, 2020 link archive General
As many people in the general population are not familiar with what viruses are and what they look like, the University of Hong Kong has released a short video on the new novel Coronavirus growing in culture.
youtube.com [2022-07-31] HKUMed channel, February 4, 2020 link archive General
Enjoy this conversation between host Doug McKenty and two powerhouses on the cutting edge of science, Dr. Judy Mikovits, a virologist who lead the team that isolated XMRV, and Dr. Stephanie Seneff who has been focusing her work on the ubiquitous toxin glyphosate. Individually, both scientists bring vast knowledge and objectivity to their areas of expertise. Together, they represent a vast comprehension of the scientific process that brings humanity to the limits of our collective understanding of how the world works. This discussion includes a deep dive into the quickly evolving science behind the functioning of the human virome and posits a theory of health and disease that revolves around modern theories concerning how virus’ work inside the body. Their ideas focus on immune system health, rather than outdated concepts of viral eradication. Find out more about Dr. Mikovits at http://plaguethebook.com/ and Dr. Seneff is on the web at https://stephanieseneff.net/
Claims made by Andrew Kaufman and Tom Cowan in response to statements I’ve made about the whole genome sequencing of SARS-CoV-2 are incorrect.
[...]
Introduction
In a typical piece of hate mail that landed in my email inbox in mid-July, an angry reader called me “ignorant” and “stubborn” for saying that SARS‑CoV‑2 exists while alerting me to a video published on July 13, 2022, by Dr. Tom Cowan, a leading proponent of the claim that it does not. In the video, which my fan evidently found persuasive, Cowan responds to something I had written about the whole genome sequencing of SARS‑CoV‑2 and purports to explain why I was wrong. However, it is Cowan who is wrong and continues to misinform his audience about the existence of the coronavirus that causes COVID‑19.
Although Cowan was unaware of the origin, the specific quote of mine to which Cowan responds in the video was something I wrote in an email newsletter on June 16. In that email to my subscribers, I responded to an article written by Dr. Andrew Kaufman, another leading proponent of the claim that SARS‑CoV‑2 does not exist, in which he similarly attempted but failed to debunk statements I had made in an interview with journalist Bretigne Shaffer about counterproductive misinformation emanating from within the health freedom movement. (That interview was later cited by Dr. Joseph Mercola in an article at Mercola.com in which he expressed his agreement with my viewpoint, which is probably how Kaufman came to learn of it.)
As an example of how Kaufman attempted but failed to rebut my statements in that interview, he resorted to strawman argumentation, such as attributing to me the claim “that scientists do not yet have the technology to purify viral particles”, which he then rebutted by saying that they do. But that is a lie. I never said any such thing.
The rest of his arguments were of a similar nature, either logically fallacious or factually incorrect, as I discussed in my newsletter but will not get into here except for the part that’s relevant to Cowan’s rebuttal video.
Here is that relevant excerpt from Kaufman’s article:
Hammond claims that scientists can do genetic sequencing of the particles found in tissue cultures. . . . Hammond describes the method accurately, in that they start with lots of pieces of genetic material, and then a computer does sophisticated calculations and simulations to put them together. The problem—which Hammond does not describe—is that the starting material for these experiments is not a pure organism; it’s not just a virus. . . . [T]here are many sources of genetic material. When they put those little bits of genetic material into the computer, the computer doesn’t know which organism they’re from—since they are not starting with a pure virus, there’s no way to tell.
Kaufman is incorrect.
First of all, it isn’t true that scientists never purify a sample prior to doing whole genome sequencing. Depending on the type of sequencing being done, it may or may not be necessary to first isolate the virus. A typical process would be to purify the patient sample with filtration or centrifugation, inoculate cell culture with the supernatant and watch for viral replication and cytopathic effects in comparison to an uninoculated control, observe the virus under an electron microscope, and utilize whole genome sequencing technology to place the virus on its evolutionary family tree.
“PCR positive faecal samples(in 200 ml buffer) were gradient centrifuged at 3,000–12,000g and supernatant diluted at 1:10 in DMEM before being added toVero E6 cells.”
“Virions from a 10-ml culture were collected, fixed and concentrated/purified by sucrose gradient centrifugation.”
“Purified virions displayed typical coronavirus morphology under electron microscopy.”
On March 20th, members of The Last American Vagabond team gathered for a 6 hour fundraiser. During the conversation Derrick Broze asked the team of Matthew Ehret, Whitney Webb, and Ryan Cristian where they stand on the existence of COVID19.
theconsciousresistance.com [2023-03-22] Derrick Broze, Matthew Ehret, Whitney Webb, Ryan Cristian, March 20, 2023 link archive General
The declaration calls for individuals at significantly lower risk of dying from COVID-19 – as well as those at higher risk who so wish – to be allowed to resume their normal lives, working normally at their usual workplaces rather than from home, socialising in bars and restaurants, and gathering at sporting and cultural events. The declaration claims that increased infection of those at lower risk would lead to a build-up of immunity in the population that would eventually also protect those at higher risk from the SARS-CoV-2 virus. The declaration makes no mention of physical distancing, masks, tracing, or long COVID, which has left patients suffering from debilitating symptoms months after the initial infection.
Dr Martin Kulldorff is an American statistician, epidemiologist and Professor of medicine at Harvard Medical School.
During an extremely important time with regard to the unfolding of the Covid-19 narrative, Dr. Martin Kulldorff joins us to explain in detail why the current policy response of lockdowns and restrictions may actually be doing more harm than good. Highlighting the benefits of allowing the younger generations to achieve some level of herd immunity and protecting the vulnerable and elderly as the wisest approach.
[...]
Alongside Dr. Sunetra Gupta, Professor of theoretical epidemiology in the department of zoology at Oxford University and Dr. Jay Bhattacharya, Professor of medicine and economics at Stanford University, they have constructed, The Great Barrington Declaration.
A heavily debated and considered petition calling on those in the corridors of power to reformulate their response to the pandemic and put an end to the blanket lockdowns crippling the economy, destroying businesses and damaging the physical and mental wellbeing of our citizens. They have called for Focussed Protection and suggested that young adults and children, the least affected by the virus, be allowed to continue their lives without restriction. That the elderly and most vulnerable members of our society should be shielded from exposure and protected from a virus risk they state has a thousandfold difference between the oldest and youngest.
[...]
freedomplatform.tv [2021-04-19] Brian Rose & Dr. Martin Kulldorff, November 11, 2020 link archive General
More information on Great Barrington Declaration
- Coronavirus Whistleblowers -
Several doctors, nurses and other professionals have stepped forward, risking their jobs and livelihoods calling out the medical establishment, government officials and main stream media for their mishandling of the COVID-19 pandemic and outright lies they're telling the public.
The following is a set of questions that I have put together for those who are still “sitting on the fence” and who might be persuaded to do their own research. It is, for that reason more conservative than my own personal position.
thewallwillfall.org [2021-02-09] February 9, 2021 link archive General
Guided by the meticulous work of Dr. David E. Martin, Plandemic II: Indoctornation, tracks a three decade-long money trail that leads directly to the key players behind the COVID 19 pandemic.
Plandemic II will connect the dots between all forms of media, the medical industry, politics and the financial industry to unmask the major conflicts of interests with the decision-makers that are currently managing this crisis.
Frauds related to the CoVid Con include the following:
1) we’ve never seen this before 2) there is no safe, effective treatment 3) CoVid is deadly to all 4) you’re a “case” and “infected” even if you have no symptoms 5) asymptomatic “super spreaders” are a problem 6) the tests are scientifically sound 7) all respiratory problems are likely CoVid cases 8) masks protect your health 9) the lockdowns reduced death rates 10) intubation and venting is a reasonable response to the symptoms
has been used in an absolutely unscientific, manipulative and deceptive way to justify this manufactured coronavirus crisis, which the evidence shows is a fake pandemic. The international lockdown which covers around 100 nations and at least 20% of the world right now is based upon the idea that there is a new distinct virus SARS-CoV2 which is spreading, infecting and causing the disease COVID-19. However, there are many key foundational questions which cannot be adequately answered. The most important of these is that the virus itself has never been isolated nor thoroughly proven to be causing the disease (or more accurately diseases) that people have! This is in addition to the obvious manipulation of the figures with false positives and other sleights of hand such as inflating the numbers by counting anyone who merely had the virus as “dead from” the virus. The coronavirus fails Koch’s postulates. The Emperor has no clothes – and all the power grabs and emergency decrees are based on lies. We are not looking at 1 virus, 1 cause and 1 disease; we are looking a cluster of diseases and a variety of causes, hidden by the COVID-19 umbrella term to fuel the fake pandemic narrative.
thefreedomarticles.com [2021-01-15] By Makia Freeman, April 8, 2020 link archive General
CDC (Center for Disease Control) scientists made some COVID admissions
that totally destroy the official COVID narrative in a study published in June 2020 entitled Severe Acute Respiratory Syndrome Coronavirus 2 from Patient with Coronavirus Disease, United States. The interesting thing about this whole scamdemic is that when you dig deep enough, the truth is out there – and it is admitted by official sources – however it does take a lot of persistence to cut through the propagandistic maze of disinfo. In this article, we’re going to take a look at the significance of what the CDC scientists revealed, namely that for their research involving the allegedly new virus SARS-CoV-2, they only used 37 base pairs from actual sample tissue and filled in the rest (around 30,000 base pairs) with computer generated sequences, i.e. they made it up! The other of the COVID admissions is equally as stunning: after testing they found that SARS-CoV-2 could not infect human tissue.
#1 COVID Admission: The Computer-Generated Frankenstein Virus: CDC Scientists Admit Only Using 37 Base Pairs from Real Tissue to Assemble SARS-CoV-2
#2 COVID Admission: CDC Scientists Found that SARS-CoV-2 Didn’t Infect Human Tissue
[...]
These 2 COVID Admissions Sink the Official Narrative Even More
So there you have it: more scientific fraud in the form of these 2 COVID admissions, and yet more evidence showing there is no real virus, and whatever the ‘virus’ is, it certainly not anything to be worried about if you are a human – which I guess you probably are if you’re reading this. These COVID admissions go to show that the truth is often hidden in plain sight, and that people in positions of power must always be carefully scrutinized. We must apply critical thinking to everything that comes from official sources.
thefreedomarticles.com [2021-01-15] By Makia Freeman, October 26, 2020 link archive General
Richplanet proudly presents the latest film by U.S. film maker Chris Hampton of Wolf Clan Media. The film delves deeply into the companies, individuals and families who have profited from the global pandemic scam. He exposes a complicated web of global power, which leads largely to Switzerland and also to Italian black nobility families. The film features an interview with Iain Davis who was featured on Richplanet show 290.
More information (and link to part 2) at source: richplanet.net
Note: Many broad claims are made here. Throughout this article, sources are provided for articles that provide the evidence to substantiate these claims.
The most plausible explanation for this inexcusable behavior was that oligarchs like Bill Gates chose to copy the playbook Fauci used throughout the early days of AIDS. At that time, highly effective treatments for AIDS were kept away from the public so that highly lucrative and extremely dangerous drugs could instead be forced upon a desperate population, resulting in many homosexual men being sacrificed to enrich a small number of predatory oligarchs.
In the case of COVID-19, remdesivir, a dangerous and ineffective (but highly lucrative) medication initially occupied that niche. Aided by the relentless efforts of corrupt members of the federal government, remdesivir was given a monopoly over hospital care for COVID-19 patients. Through its abysmal failure to cure the disease, remdesivir set the stage for "emergency" vaccines to enter the market, an “emergency” that only existed because effective treatments were kept out of the hospital system thanks to remdesivir’s monopoly.
Due to the emergency nature of COVID-19, many necessary vaccine development steps were skipped, and a few extremely questionable vaccines were allowed to enter the market. Because individuals, such as Bill Gates, who invested large amounts of money in the COVID-19 vaccines, also held significant financial influence over the media and tech platforms, none of these red flags were ever brought to the public's attention, and the vaccines were instead hailed as the second coming of our lord and savior.
Once it became clear the vaccines were both unsafe and ineffective, all of the institutions that promoted the vaccines instead chose to aggressively censor any suggestion the vaccines could be harmful and engaged in a variety of highly manipulative tactics to force the public into taking as many vaccines as possible. As a result, an incalculable degree of damage has occurred and I suspect that we have still only seen the tip of that iceberg.
For science to function, an open debate is required. Unfortunately, in recent years (I believe this change was initiated during Obama's presidency) support of the scientific process has been replaced with blind faith in things claiming to be “science" even though they do not follow the scientific process. Since that process was not followed throughout the pandemic, many atrocious policy decisions were allowed that resulted in disastrous outcomes for millions. This has created a widespread mistrust of countless institutions that have remained mostly unchallenged for decades, and it is my sincere hope the political will now exists for a once-in-a-lifetime opportunity to reform some of them.
There were many serious potential issues with the COVID-19 vaccines which were identified long before the vaccines came to market, yet due to the climate of corruption within the government, routine stifling of scientific debate, and mass censorship, none of these concerns were addressed before the vaccines entered the market.
I and many others lacked the immunological expertise and access to proprietary “data” scientists within the major vaccine manufacturers had. Despite this, each of us was able to independently predict exactly what issues would emerge with the vaccinations. Because of this, I must assume that the issues were also known ahead of time by the vaccine manufacturers.
For example, from the start, it was apparent that the vaccines would be ineffective in preventing COVID-19 (there was a lot of ignored evidence suggesting this was the case) and it was suspected the vaccines would cause the virus to rapidly mutate into variants the vaccines did not cover, thereby destroying what little efficacy the vaccines did have. Before we go further, I would like to request that you review this remarkable two-minute video, especially in light of the fact it was made over a year ago.
Here are the top 10 major events that took place in relation to COVID in 2023.
COVID-19 in 2023 has been full of revelations and controversy.
Most health leaders involved in the U.S. pandemic response have resigned or been replaced, with one leaving his agency with a study that received much fanfare for a somewhat controversial take on vaccines.
Compared to 2022, the science on the effectiveness and risks of masking and vaccinations has become increasingly clear with the release of highly authoritative studies this year.
Let us review the top 10 major events that took place in relation to COVID in 2023.
1. FDA and CDC Find More COVID Vaccine Adverse Events, Including Stroke
[...]
2. Vaccines Cannot ‘Effectively’ Control COVID: Fauci After Resigning
[...]
3. Gold Standard Review Finds Evidence of Masking ‘Uncertain’
[...]
4. Repeated Vaccination Weakens the Immune System, Studies Suggest
[...]
5. DNA Contamination Detected in mRNA Vaccines, and FDA’s Response
[...]
6. COVID Vaccine-Injured People Compensated
[...]
7. Doctors Can Prescribe Ivermectin: FDA Lawyer
[...]
8. Mask Mandates Return in August, New COVID Vaccines Approved
[...]
9. Final Batch of Pfizer Vaccine Documents Released by the FDA
[...]
10. Not Messenger RNA but Modified RNA, Vaccines Form Aberrant Proteins
[...]
theepochtimes.com [2023-12-28] Marina Zhang, December 26, 2023 link archive General
Ep. 60 Is the lesson of the Covid disaster that we should give its architects more power? Bret Weinstein on the WHO’s plans for you. pic.twitter.com/ku3O5BdeoF
Bret Weinstein makes the salient point that the entire plot was foiled by the sheer number of dissidents that were there from the beginning and grew over time. These, he said, shocked the creators of this industrial scheme, because they figured that they had the media, government, and big tech all wrapped up in a bow and that no serious dissidence would ever happen. The ranks of the dissidents grew and grew for two years and reached the multitudes in popular podcasts and writings, as well as new institutions such as Brownstone.
Bret says this is success but it also portends something terrible in the future. In the next go-round, says Bret, the powers that be want to make sure that there is not a repeat. The censorship will be tighter, and the penalties for going against the government’s plan will be more severe. They have learned from this experience, and their takeaway is not that such absurdities didn’t work but that they were too lenient this time around. They plan to make sure that this doesn’t happen next time.
Here we get to the World Health Organization, which has issued a fatwa against disinformation and has greenlighted censorship on a global level. YouTube and Google are already captured and doing the institution’s bidding, as is the European Union. They will use the next several years to tighten the screws and get every nation roped into a pandemic accord that will obligate every government to censor and vaccinate one way or another. In other words, they have learned nothing except for the wrong lessons.
This was probably the most intuitively correct and ominous part of the entire interview.
Naively, many of us figured that after this awful experience with lockdowns, masks, and mandates that such would never be attempted again. But that is not where we are today. There is a reason we haven’t heard any high-profile apologies or admissions of wrongdoing. The reason is that there was never a purpose to do the right thing. It was an industrial takeover from the beginning, a perfect corporatist scheme for gaining a major advantage in the wars for pharmaceuticals and their future. The rest of the “Great Reset” was just taking advantage of the ensuing chaos.
They're using the phantasm of a horrible new plague to wipe out national sovereignty & human rights—not for a finite lockdown, as in 2020, but forever, with dissidence an outright criminal offense
twitter.com [2024-01-07] Tucker Carlson interviews Bret Weinstein, Jan 6, 2024 link archive General
As the establishment begins signaling new COVID measures (well, the same old measures deployed before), it is up to We The People to use our resilience to push back and not comply
[...]
I’m sitting here watching all of the news headlines and the establishment setting up the narrative that the only way to deal with this “uptick” in “COVID” cases is to implement all the same nonsense that was implemented back in 2020 and beyond.
Well, they might have a huge problem with that.
We can all remember a time, it seems like it was only yesterday, when the fear campaign began revving up. I remember very clearly in the late winter, going into Spring of 2020, watching the news that some “virus” was making its way across the world from China and that we all needed to be very afraid.
[...]
tlavagabond.substack.com [2023-08-24] The Last American Vagabond, Scott Armstrong, August 23, 2023 link archive General
Last year, President Biden announced that COVID was over, or at least he declared we were on a promising path to defeating the virus. Despite the sense of optimism, the media seems to be prepping for a COVID “comeback tour.” Yes, you heard that right—COVID is reemerging as a major threat this fall, according to news outlets and the Biden administration. But how much of this should we take at face value?
First, let’s scrutinize the facts and numbers.
According to the Centers for Disease Control and Prevention (CDC), COVID cases have increased four weeks in a row. But hold on. What the mainstream media, like NBC News, isn’t telling you is that COVID-19 follows seasonal and regional patterns.
“NBC News is deceiving you,” rebuked Jesse Watters, “by denying you the real reason there’s a tiny uptick in cases. COVID follows seasonal and regional patterns. Every year, there [are] three waves. One starts in New England in the spring, the second travels north from Mexico in the summer, and the third wave travels in all directions from the Dakotas in the fall.”
[...]
vigilantnews.com [2023-08-24] The Vigilant Fox, Aug 23, 2023 link archive General
The Devil's favorite doctor is now popping up again, to help roll out "Pandemic 2" (in hopes of getting millions "vaccinated" even MORE, while forcing "vaccination" on the rest of us)
He’s back to tell us that “we are not done with COVID”—as “we know,” he says, because of the (imaginary) number of “new cases” breaking out worldwide.
(While his say-so will undoubtedly convince all those who are still stupefied by fear, what we know is that all those “new COVID cases” are, in fact, not COVID cases, but the countless deaths and disabilities caused by the COVID vaccination drive.)
The state wants local organizations to distribute promotional materials and help hold events to promote the COVID jabs.
(LifeSiteNews) — The Mississippi State Department of Health (MSDH) is offering businesses and churches money in exchange for promoting COVID-19 vaccination despite persistent doubts about the need and safety of the shots.
On Monday, MSDH announced via social media that businesses and faith organizations can receive $1,000 for participating in the state’s Communities Conquering COVID vaccination education program.
“The program will train representatives from barbershops, salons, churches and faith-based organizations as community health advocates to provide vaccination education and materials to their members and clients,” the announcement says. In addition to training, the post says participants will distribute COVID test kits and vaccination material, and help with local vaccination events.
[...]
lifesitenews.com [2023-08-26] Calvin Freiburger, August 24, 2023 link archive General
Mass media is calling for the reinstitution of COVID restrictions due to new variants, with no conversation about the efficacy or the harm they’ve caused. Jefferey Jaxen connects all the dots, which appears to be pointing to a Pandemic 2.0.
Will You comply with Pandemic 2.0? As mainstream media pumps out another campaign of fear over new COVID variants, social media has made it very clear ‘we the people’ will not comply with unscientific lockdowns, mandates, or masks again.
thehighwire.com [2023-08-29] The HIGHWIRE, August 24, 2023 link archive General
Classes at Runge ISD will resume on Tuesday, Aug. 29
RUNGE, Texas – A school district in South Texas is closing temporarily after seeing a surge of COVID-19 cases among students and staff members.
The superintendent of Runge ISD announced in a letter Monday that schools will be closed from Tuesday, Aug. 22 through Friday, Aug. 25.
“The safety and well-being of our students, staff, and community is a top priority,” Superintendent Hector Dominguez Jr. said in a statement.
Runge, Texas is in Karnes County and is just under an hour and a half away from San Antonio.
The school district updates its COVID-19 case numbers on its website frequently. As of Aug. 21, the district had 10 active cases among staff members.
In addition to the school closures, all extracurricular activities and practices will also be canceled out of precaution.
Students and staff can return to the classroom at 7:50 a.m., Tuesday, Aug. 29.
“Please be advised that a new instructional calendar will be presented soon, indicating new instructional dates for students,” Dominguez said in the letter.
? It used to be that neurotic, OCD people were obsessed with their own bathroom habits. But it’s a brave new post-covid era, and OCD people have expanded their horizons; they are now equally fascinated with your number-two habits. This bathroom biofeedback story, which you probably never heard of, is the biggest thing going in the Covidian world, and it is threatening to break through as a mainstream Narrative.
So let’s shut it down!
First, here is just one (of very many) example to set the hysterical tone. This particular Covidian heart-breaker has 23,000 Covidian followers:
I keep thinking they’re running out of words and they keep coming up with new ones. Last year it was the dark winter of suffering and deaths, and this year it’s the harrowing year of heartbreak. Or something.
Covidians’ biggest problem is that all the daily covid dashboards have been unplugged, shut down, and de-funded, and worse, mandatory covid reporting has expired too. That just leaves them with one place to look to sustain their neurotic habits: our poo. The levels of scatological obsession are not just rising in social media’s toilet bowl, either. The levels of poop-obsessed neuroses are also surging with corporate media maniacs like Newsweek.
And even the big papers. Here’s another example, from yesterday’s Boston Globe:
Before you ask, the “brung back mask mandate” was not new; it’s a standing Mass General policy triggered by a very small percentage (2.85%) of emergency visits from any respiratory virus. Mass Gen just reached 2.85% for the first time this fall, and — following its existing policy — said it will require workers to mask starting January 2nd. Now check out this next sentence the Globe slipped into its story way down the page: “Last year, local hospitals experienced respiratory infection levels as high as 7.3% during what many health officials called the tripledemic.”
So … yawn … this year’s “surging” 2.85% respiratory ED burden at Mass General is half of last year’s burden. Wait! I think I just saw the North Star while my eyes were rolling straight up. Anyway, this isn’t just another stupid, fear-peddling non-story about covid. Remember the wastewater. Here’s what the Globe said about that not-for-the-dinner-table subject:
The Boston-area COVID wastewater data keeps spiking. The COVID wastewater data is the first sign of virus cases in the community. The south-of-Boston virus wastewater weekly average was up to 1,611 copies per milliliter ahead of Christmas, which is nearly double from early December. The 1,600-plus average is the highest the COVID wastewater data has been since January.
The north-of-Boston average was up to 1,150 copies per milliliter ahead of Christmas — also about double from earlier this month. The 1,100-plus average in the north is also the highest since January.
See what the Globe did there? The wastewater levels — copies per millileter? What? — are the highest they’ve been sincelast January.
Um, just now we’re one week from January. So they’re just reporting normal, seasonal covid levels. It’s literally a non-story. But the poor Covidians have been convinced by all this fake news hysteria that this is the big one. They have poo dashboards and post-digestive tracking systems and they are utterly fascinated by the things they can find at the end of their plumbing. Even the CDC is now offering a National Wastewater Surveillance System — with its own acronym, of course, the slightly-unwieldy but official-sounding NWSS, which at your option can either be pronounced news or noose, which rhymes with loose, as in loose bowels.
And loose bowels are just the ticket for getting the best readouts. “See the data and take action to protect your health,” says the CDC’s website for the NWSS. Don’t poo-poo it. People can take lots of actions after plumbing their sewage data. The imagination boggles. But it’s good to see the CDC finally digging into the pandemic with both hands.
This might possibly be the most insane OCD to run down the pandemic’s sewer system so far in a long diarrheaic stream of pandemic psychosis. Covidians readily admit — but then promptly ignore — that current seasonal covid wastewater levels are but a tiny fraction of the January 2022 peak:
The “bottom” line is, there’s nothing suggesting anything remarkable about the winter covid levels in the sewers. Nothing that justifies masking. And, contrary to all the headlines and the flailing Narratives, there is no re-masking movement developing.
So, you ask, why are Covidians — the science followers! — so exercised? I’ll tell you, but you won’t believe me. It’s because they still believe in Zero-Covid. And they think the entire world should be focused on achieving that unreachable goal, just like they are, even if it requires anal-ytically plumbing the depths of defecation along with them.
coffeeandcovid.com [2023-12-30] Jeff Childers, December 29, 2023 link archive General
? Question asked! The New York Times reporters are just obsessed with Americans’ bathroom habits. The Gray Lady ran a scatalogical story yesterday (non-paywalled!) headlined, “We Are in a Big Covid Wave. But Just How Big?”
(That’s what she said.)
It was another unintentionally hilarious feces-focus story, and in a sane world the conversation about wastewater testing as anything but a fetid fetish should be over. The sub-headline seemed to recognize the thin ice over the septic pond, admitting “Wastewater data has become perhaps the best metric to track the spread of the virus in the U.S., but it’s an imperfect tool.”
Bwahaha! Read the fine print under the chart again. I defy you to explain what on Earth this is supposed to mean:
Note: the C.D.C. calculates a viral activity level for each testing site as the number of standard deviations above a baseline, set at the 10th percentile of the normalized viral RNA concentration data. The national estimate is the median activity level for sites with at least six weeks of data.
Remember — the Covidians are clutching their wastewater data the way a hypochondriac hangs onto two months of carefully-collected stool samples. The article recognized this, acknowledging “For many who remain at higher risk from the virus — like those who are older, immunocompromised or already have a serious illness — it’s become a crucial tool helping them understand when to be particularly careful.” It’s all they have left! The other measurements have let them down. Disappointingly, as the article admitted, covid “hospitalizations and deaths have remained far lower than in previous years.”
So without wastewater estimates, it would be all over, time to take off the mask. Which is a terrifying nightmare for your average Covidian.
The sub-headline euphemistically called the viral-load estimates “imperfect.” How imperfect? Well, first — as that inscrutable disclaimer indicated — they lack data from everywhere. They only have it from a few testing sites. Just how many is a closely-guarded secret. Nobody’s saying how many sites are included; whatever that number is, it appears to change from week to week. That’s why they extrapolate the national figure.
Meaning, they’re guessing. Again.
But the, um, lack of precision gets even worse. Wastewater testing is doo-doo voodoo. Here are the various problems described at various points in the article, which I edited together:
(Wastewater testing is) an imperfect metric, useful primarily for identifying if there’s an acceleration of virus spread, not for telling you exactly how much virus is circulating. The data is often reported as normalized viral copies per milliliter or per gram, a number that is nearly impossible to translate into precise case counts. And the C.D.C. doesn’t show the actual concentration levels — its dashboard instead shows how much they have increased relative to when spread was low.
The amount of RNA in a sample will fluctuate depending on many factors, including the local population at any given time — think of a holiday influx into Miami or a college town emptying out for summer — and how much other material, such as industrial waste, is in the system. A peak in the data may not mean exactly the same thing this year as it did last year.
And nationwide estimates can be tricky. The data excludes people with septic tanks and cities with no wastewater testing. There can be data lapses, as when the C.D.C. switched contractors last year. Existing sites can stop testing, and new sites start up, as the network changes and expands.
Finally, there are changes to the virus itself that could make comparisons over time more difficult. Scientists say there are hints that this latest variant, JN.1, may be able to better replicate in the gut. It could mean that infected people shed more viral copies than they used to, (making the) same number of infections look like a lot more Covid.
Sounds great. By “great,” I mean completely unreliable. What does the Times suggest Covidians do with all these stinky problems that make wastewater testing look like a pile of BS? Here is the country’s top newspaper’s scientific suggestion:
Many experts who study this data recommend dropping any notion of precision and just squinting a little at the line’s recent trajectory.
Just squint at the wastewater data! No, not that much. If you squint just right, you might even start to believe.
coffeeandcovid.com [2024-01-12] Jeff Childers, January 11, 2024 link archive General
In order to combat the media bias regarding public health during the COVID-19 crisis, we are asking for volunteers to help us with a reference project. We believe that it is time to put together the definitive list(s) of harms done by the disastrous public health policies during the past three years. Unless we are able to rigorously document the mistakes made, the same policies will be forced upon us again. When the next administration takes office in 2024, we must have the receipts to make sure this never happens again..

 / COVID-19")

 after he collapses in Wuhan, China.")